
CONGENITAL CLUBFOOT
CONGENITAL CLUBFOOT Congenital Talipes Equino Varus (CTEV)
- ‘Clubfoot’ is a rather vague term.
- Used to describe a number of different abnormalities in the shape of the foot.
- Commonest congenital foot deformity i.e., Congenital Talipes Equino Varus (CTEV).
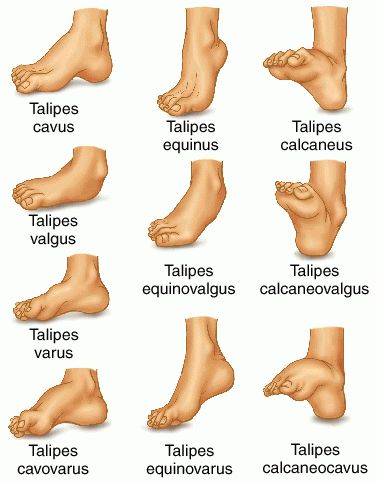

Equinus: (derived from ‘equine’ i.e., a horse who walks on toes).
- This is a deformity where the foot is fixed in plantar-flexion.
Varus: The foot is inverted and adducted at the mid-tarsal joints so that the sole ‘faces’ inwards.


AETIOLOGY
- Aetiology is not known, hence it is termed idiopathic.
- In others, the so called secondary clubfoot.
1. Idiopathic clubfoot:
- Mechanical theory: The raised intrauterine pressure forces the foot against the wall of the uterus in the position of the deformity.
- Ischaemic theory: Ischaemia of the calf muscles during intrauterine life; leading to foot deformities.
- Genetic theory: Some genetically related disturbances in the development of the foot held responsible for the deformity.
2. Secondary clubfoot:
- Paralytic disorders:
- Arthrogryposis multiplex congenita (AMC)
Foot examination:
- Normally, the foot of a newborn child can be dorsiflexed until the dorsum touches the anterior aspect of the shin of the tibia.
- This is a good screening test for detecting the milder variety of clubfoot.
- The more classic one will have the following findings:
Bilateral foot deformity in 60 per cent cases.
Size of the foot smaller (in unilateral cases).
• Foot is in equinus, varus and adduction.
- This can be judged by the inability to bring the foot in the opposite direction.
- In late cases, in addition, cavus of the foot may also be present.
Heel is small in size; the calcaneum may be felt with great difficulty.
Deep skin creases on the back of the heel and on the medial side of the sole.
Bony prominences felt on the lateral side of the foot, the head of the talus and lateral malleolus.
Outer side of the foot is gently convex; dimples on the outer aspect of the ankle.
- A patient of residual polio may present with equino-varus deformity, which may mimic clubfoot,
- but there will be paralysis of some other part of the limb.
- Presence of sensory deficit points to an underlying neurological cause.
- The presence of deformities at other joints indicate possible arthrogryposis multiplex congenita (AMC).
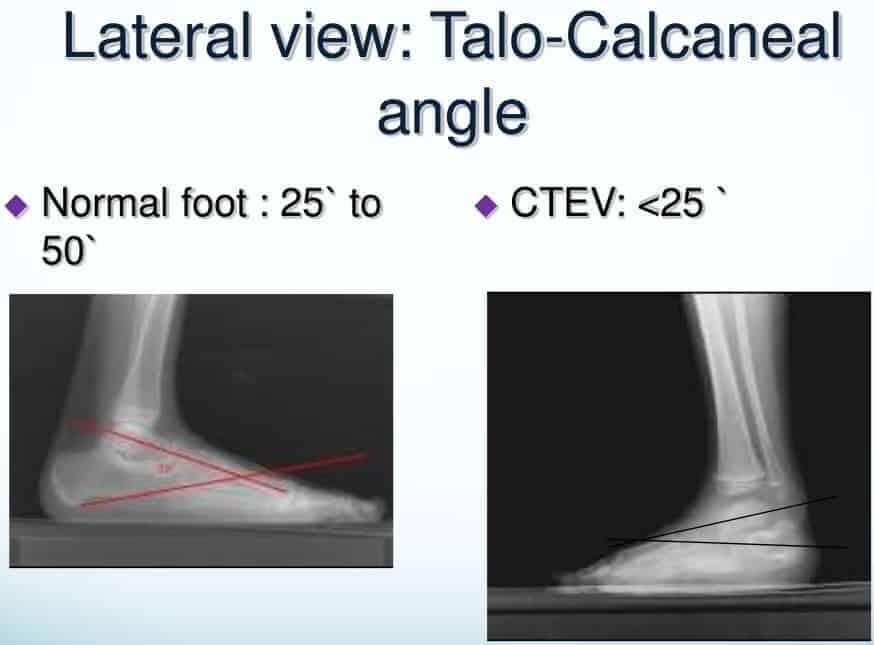
- The talo-calcaneal angles in a normal foot are more than 35.
- In CTEV these are reduced.



1. Manipulation alone
2. Manipulation and PoP
- Kite’s philosophy
- Ponsetti’s philosophy
- Postero-medial soft tissue release (PMSTR)
- Limited soft tissue release
- Tendon transfers
- Dwyer’s osteotomy
- Dilwyn Evan’s procedure
- Wedge tarsectomy
- Triple arthrodesis
- Ilizarov’s technique
- CTEV splints
- Denis-Brown splint (DB splint)
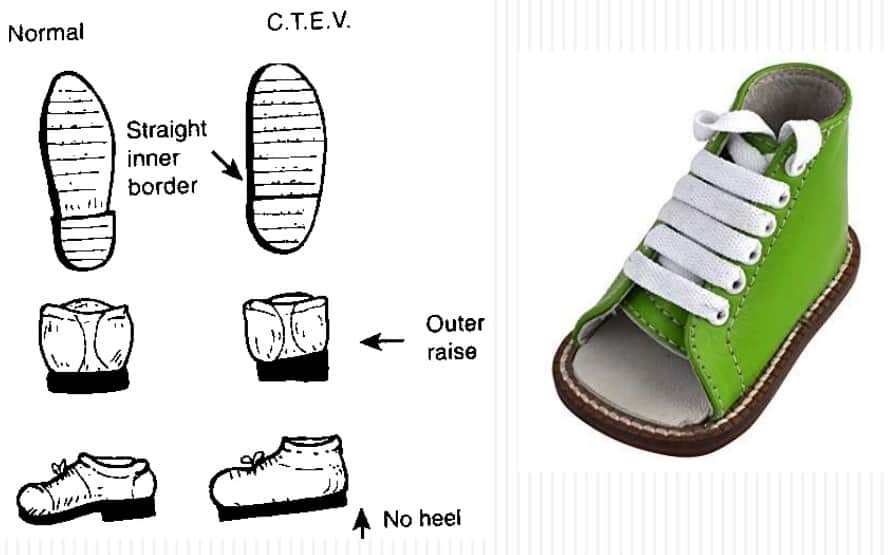
- CTEV shoes



Exam Important
- Most common cause of CTEV is Idiopathic.
- The typical deformity in CTEV is Ankle equinus, Subtalar inversion & Forefoot adduction
- Treatment for a newborn child with CTEV is Manipulation and strapping or serial cast.
- Treatment of partially corrected CTEV with cavus deformity is Plantar release.
- Early congenital talipes equinovarus (CTEV) is treated by Manipulation and corrective splint.
- Splint used in CTEV after correction is Dennis Brown splint.
Click Here to Start Quiz

