
ECTOPIC PREGNANCY
DEFINITION:

- An ectopic pregnancy is one in which the fertilized ovum is implanted and develops outside the normal endometrial cavity.
- The cause of fetal death in ectopic pregnancy is postulated as Vascular accident
- In Interstitum part of fallopian tube longest survival
SITES OF IMPLANTATION:

TUBAL PREGNANCY:
ETIOLOGY:
- Salpingitis and pelvic inflammatory disease (PID)
- Genital tuberculosis
Iatrogenic:
- Contraception failure(least with condom)
- Tubal surgery
- Intrapelvic adhesions
- ART
Others:
- Previous ectopic pregnancy
- Prior induced abortion
- Developmental defects of the tube
- Transperitoneal migration of the ovum
RISK FACTORS:
- History of PID
- History of tubal ligation
- Contraception failure
- Previous ectopic pregnancy
- Tubal reconstructive surgery
- History of infertility
- Calendar method
- ART particularly if the tubes are patent but damaged
- IUD (Progestasert)use
- Previous induced abortion
- Tubal endometriosis
MORBID ANATOMY:
CHANGES IN THE TUBE:
- Implantation in in between two mucosal folds.
Decidual change:
- Muscles undergo limited hyperplasia and hypertrophy
- Blood vessels are engorged
- Intramuscular implantation
- Pseudocapsule
- Blood vessels are eroded
- Blood accumulates in between the blastocyst and the serous coat
- Hemoperitoneum
CHANGES IN THE UTERUS:
- Endometrium sloughs out causing uterine bleeding.
- Decidual cast:decidua is expelled as a single piece through the cervix
CLINICAL FEATURES:
ACUTE ECTOPIC:
- 30%
- Associated with tubal rupture or tubal abortion
Classic triad of symptoms:
- Abdominal pain (100%),
- Preceded by amenorrhea (75%)
- Appearance of vaginal bleeding (70%).
- Amenorrhea:6–8 weeks
- Abdominal pain
- Shoulder tip pain (25%)
- Vomiting, fainting attack.
- Pallor
- Features of shock
- Abdominal examination:tense, tumid, tender
- Pelvic examination
- Vaginal mucosa—blanched white.
- Extreme tenderness on fornix palpation
- The uterus Floats as if in water
CHRONIC ECTOPIC:
- Onset:insidious.
Symptoms:
- Amenorrhea:6-8 weeks
- Lower abdominal pain
- Vaginal bleeding:scanty, sanguinous or dark-colored and continuous
- Dysuria,
- Rectal tenesmus
- Rise of temperature
- Pallor
- Pulse persistently high
- Features of shock are absent.
Abdominal examination:
- Tenderness and muscle guard
- A mass in the lower abdomen
- Cullen‘s sign: Dark bluish discoloration around the umbilicus
Bimanual examination:
- Uterus often incorporated in the mass occupying the pelvis
- Extreme tenderness on movement of the cervix
DIAGNOSIS:
Blood examination:
- Hemoglobin
- ABO and Rh grouping
- TLC & DLC
- ESR
- Culdocentesis
- Estimation of ↑β-hCG
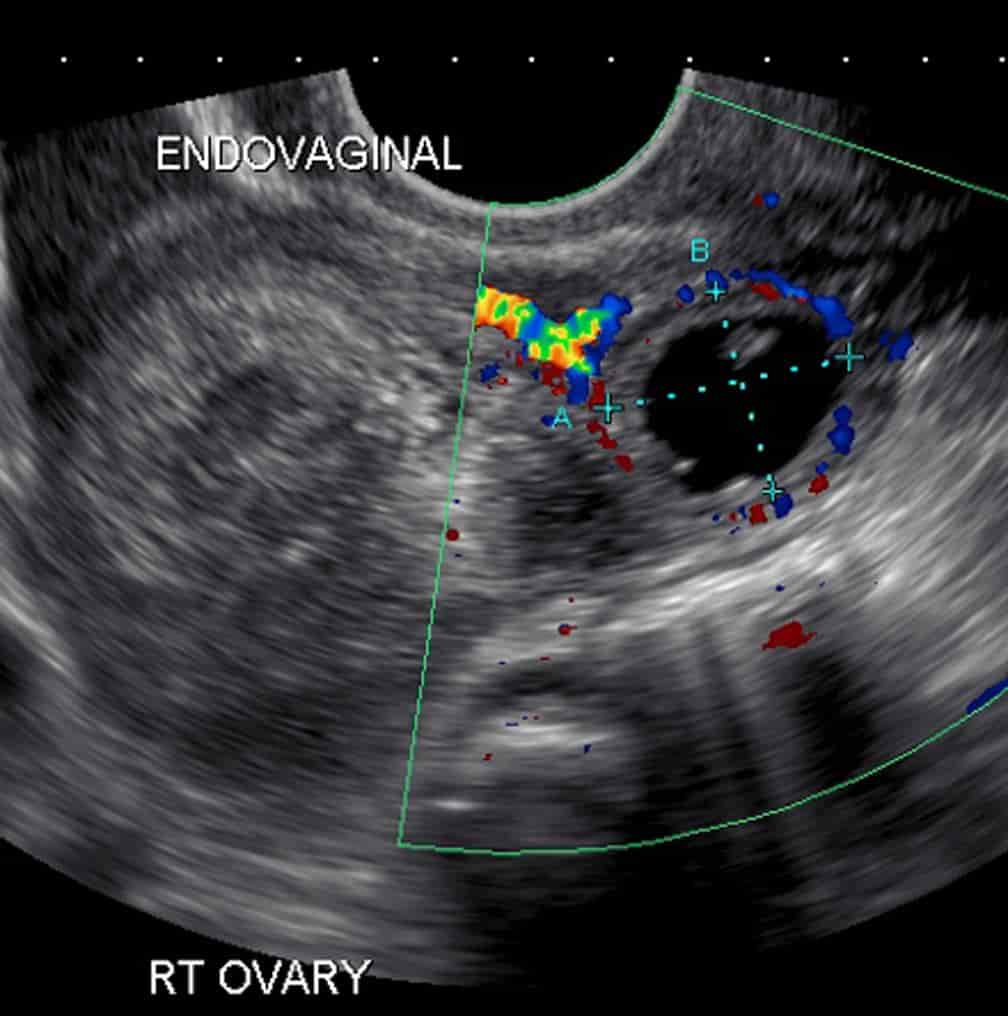
Sonography:
- Transvaginal USG(Most sensitive)
- Absence of intrauterine pregnancy with a positive pregnancy test.
- Fluid (echogenic) in pouch of Douglas
- Adnexal mass
- Rarely cardiac motion
Color Doppler Sonography:
- Ring-of-fire pattern
- Enhanced blood flow pattern
- Laparoscopy
- D & C
- Serum progesterone
- Laparotomy

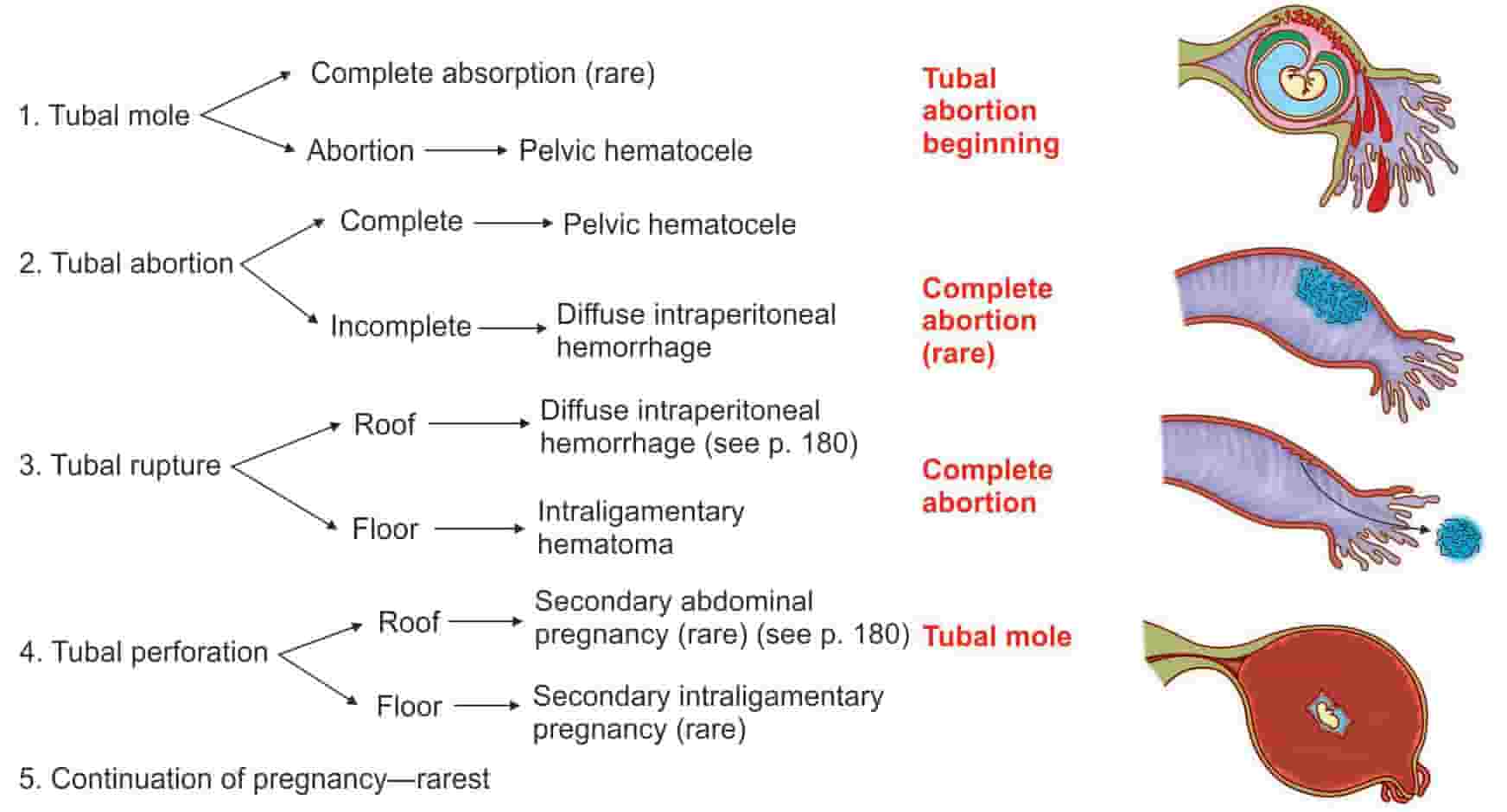
MODE OF TERMINATION:
Tubal mole:
- Repeated small hemorrhages in the choriocapsular space
The fate of the mole:
- Complete absorption
- Expulsion through abdominal ostium as tubal abortion
Tubal abortion:
- If implantation occurs in ampulla or infundibulum
Tubal rupture:
- common in isthmic and interstitial implantation
- Isthmic rupture usually occurs at 6–8 weeks
- The ampullary one at 8–12 weeks
- The interstitial one at about 4 months
Intraperitoneal rupture:
- Common.
- Rent is situated on the roof or sides
- Bleeding is intraperitoneal
Extra-peritoneal rupture (intraligamentary):
-
- Rent lies on the floor
- Isthmic implantation
Arias-Stella reaction:
- Typical adenomatous change of the endometrial glands
- Loss of polarity of cells
- Pleomorphism
- Hyperchromatic nuclei
- Vacuolated cytoplasm
- Occasional mitosis
- Intraluminal budding
- Progesterone influence

MANAGEMENT:
ACUTE:
Antishock treatment:
- Ringer’s solution
- Blood transfusion & laparotomy
- Laparoscopy :Decreased hospital stays
Laparotomy:
- Patient hemodynamically unstable
- Laparoscopy contraindicated
- Evidence of rupture
Steps:
- Abdomen is opened by infraumbilical longitudinal incision
- To grasp the uterus and draw it up under vision
- Salpingectomy
- Ipsilateral ovary and its vascular supply is preserved
- Place of subtotal hysterectomy
CHRONIC ECTOPIC:
- Laparotomy
UNRUPTURED TUBAL PREGNANCY:
Expectant management:Indications
- Initial serum hCG level less than 1,000 IU/L
- Gestation sac size less than 4 cm
- No fetal heart beat
- No evidence of bleeding
Conservative management:
- Medical management:Conservative Surgery:laparoscopically or by microsurgical laparotomy.
- hCG level is less than 10,000 IU/L & size < 4 cms
- The drugs commonly used for salpingocentesis are
- Methotrexate, potassium chloride,Actinomycin D, prostaglandin(PGF2α), hyperosmolar glucose
- Linear Salpingostomy(nulliparous woman)
- Linear Salpingotomy
- Segmental Resection
- Fimbrial Expression
- Salpingectomy
Exam Important
- The commonest complication of pregnancy after complete treatment of genital tuberculosis is Ectopic pregnancy
- Ectopic pregnancy is a reported complication of calendar method
- IUCD with highest incidence of ectopic pregnancy is Progestasert
- Condoms has the least risk of ectopic pregnancy
- In comparing laparoscopic salpingostomy vs. laparotomy with salpingectomy for the treatment of ectopic pregnancy, laparoscopic therapy results in Decreased hospital stays
- Most sensitive diagnosis test for ectopic pregnancy Transvaginal USG
- The cause of fetal death in ectopic pregnancy is postulated as Vascular accident
- Hormone responsible for decidual reaction and Arias stella reaction in ectopic pregnancy is Progesterone
- Medical treatment of ectopic pregnancy should be offered to those patients whose hCG level is less than 10,000 IU/L and the size of the mass is less than 4 cms
- 6 weeks of amenorrhoea p,pain in abdomen; USG shows fluid In pouch of douglas. Aspiration yields dark color blood that fails to clot. Most probable diagnosis is Ruptured ectopic pregnancy
- Acute abdominal pain , prolong amenorrhoea with collection of fluid in the pouch of douglas and empty gestational sac are suggestive of ectopic pregnancy
- Ectopic pregnancy is most commonly associated with Tubal inflammatory diseases
- Most common manifestation of ectopic pregnancy is Pain abdomen
- In Interstitum part of fallopian tube ectopic pregnancy will have longest survival
- Ectopic pregnancy Associated with decidual reaction
- In ectopic interstitial ring sign is seen
- Potassium Chloride, Methotrexate & Actinomycin D are used in medical management of ectopic pregnancy
- In Presence of fetal heart activity the medical treatment of Ectopic pregnancy is contraindicated
- Salpingo-oophorectomy is not done in ectopic pregnancy
- In a nulliparous woman, the treatment of choice in ruptured ectopic pregnancy is Linear salpingostomy
- Ectopic pregnancy differs from threatened abortion by that it Manifests at an early age
- Commonest cause of ectopic pregnancy is Previous salpingitis
- Causes of ectopic pregnancy includes IUCD, & Tubal ciliary damage
- Commonest site of ectopic pregnancy is tube
- Commonest type of ectopic pregnancy with rupture is Isthmic
- In a young patient with abdominal pain and feature most suggestive of ectopic pregnancy is Increase beta HCG in urine
- The most consistent sign in disturbed ectopic pregnancy is Vaginal bleeding
- The expelled products in ectopic pregnancy originate from Decidua vera
- Pathognomonic of ectopic pregnancy is Decidual casts
- Best endometrial reaction In ectopic pregnancy is Decidual reaction without chorionic villi
- Medical treatment of ectopic pregnancy is methotrexate
- Absolute contraindication to intra-uterine device is History of ectopic pregnancy
- Ectopic pregnancy is commonest in ampulla of fallopian tube
- Ectopic pregnancy can be ruled out on ultrasound by Finding foetus in uterus
Don’t Forget to Solve all the previous Year Question asked on ECTOPIC PREGNANCY
Click Here to Start Quiz
Click Here to Start Quiz

