
RETROSTERNAL GOITER
RETROSTERNAL GOITER
- Retrosternal goiter tends to arise from the slow growth of a multinodular (lower pole) down into the mediastinum.
- The nodular goiter is sucked in superior mediastinum by-
- Negative intrathoracic pressure
- Pretracheal muscles are strong in men
- Strong neck, obesity, strong ribbon muscles


CLINICAL FEATURES-
- Asymptomatic
- Dyspnea, dysphagia
- Pemberton’s sign- engorged veins of neck and chest wall (The hands are raised above the head, and the arms touch the ears)


CLASSIFICATION-
- Primary- arises from ectopic thyroid tissue in the mediastinum
- Secondary- common variety
II) According to clinical types-
- Substernal (most common type)
- Intrathoracic
- Plunging goiter
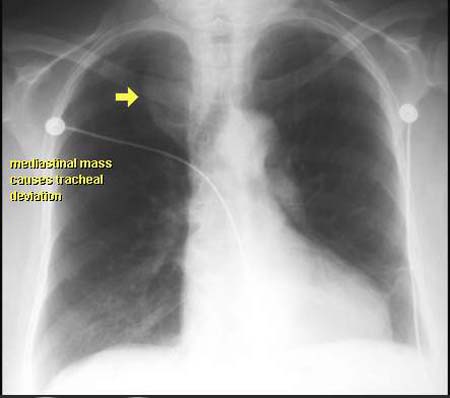
INVESTIGATIONS
- X- ray shows tracheal compression and deviation
- CT scan shows localization, size and extent.

TREATMENT-
- Surgical excision is the treatment of choice
- If gland is fixed, immobile and too large – midline stenotomy is performed
- No antithyroid drugs and radioiodine should be given to thyrotoxicosis with retrosternal goiter.
Exam Important
CLINICAL FEATURES-
- Asymptomatic
- Dyspnea, dysphagia
- Pemberton’s sign- engorged veins of neck and chest wall (The hands are raised above the head, and the arms touch the ears)
Don’t Forget to Solve all the previous Year Question asked on RETROSTERNAL GOITER
Click Here to Start Quiz
Click Here to Start Quiz

