
UTERINE PROLAPSE
INTRODUCTION:
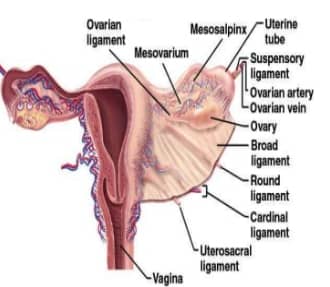


Structure supporting uterus:
- UPPER: Round Ligament, Broad Ligament(Not preventive in prolapse)
- MIDDLE:Transverse cervical Ligament or cardinal ligament(most supportive), Pubocervical & Uterocervical
- LOWER:Urogenital diphragm, Levator ani and Perineal Body

- If these muscles or ligaments stretch or become weak, they’re no longer able to support the uterus, causing prolapse. Uterine prolapse occurs when theuterus sags or slips from its normal position and into the vagina, or birth canal.
RISK FACTORS:
- Increases with woman ages as estrogen levels decrease.
- Damages to pelvic muscles and tissues during pregnancy and childbirth
- Women who’ve had more than one vaginal birth
- Postmenopausal women are at the highest risk.
- Any activity that puts pressure on the pelvic muscles
Other factors that can increase your risk for the condition include:
- Obesity
- Chronic coughing
- Chronic constipation

SYMPTOMS:
- Stress incontinency
- Feeling of sitting on a ball
- Vaginal bleeding
- Increased discharge
- Problems with sexual intercourse
- Seeing the uterus or cervix coming out of the vagina
- Pulling or heavy feeling in the pelvis
- Constipation
- Venous congestion can lead to decubitus ulcer
- Recurrent bladder infections
STAGES:
- Uterine prolapse is described in stages, indicating how far it has descended.
- Anterior vaginal wall : upper two thirds – cystocoele (Most common)
- Cytourethrocoele lower one third – urethrocoele
- Posterior vaginal wall : upper one third – enterocoele (pouch of Douglas Hernia)
- Other pelvic organs (such as the bladder or bowel) may also be prolapsed into the vagina
- Incomplete uterine prolapse: The uterus is partially displaced into the vagina but does not protrude.
- Complete uterine prolapse: A portion of the uterus protrudes from the vaginal opening.
The four categories of uterine prolapse are:
- Stage I – the uterus is in the upper half of the vagina
- Stage II – the uterus has descended nearly to the opening of the vagina
- Stage III – the uterus protrudes out of the vagina
- Stage IV – the uterus is completely out of the vagina.

TREATMENT:
Nonsurgical treatments include:
- Losing weight to take stress off of pelvic structures
- Avoiding heavy lifting
- Doing Kegel exercises, which are pelvic floor exercises that help strengthen the vaginal muscles
- Taking estrogen replacement therapy
- Reduction with tampon:Decubitus ulcer in a case of genital prolapse
- Wearing a pessary
- A device inserted into the vagina that fits under the cervix and helps push up and stabilize the uterus and cervix
- Use to treat pregnancy with prolapse
- Rubber ring passary:Used In utero vaginal prolapse
Surgical treatments include:
- Genital prolapse is best repaired after 6 months of child birth
- Uterine suspension :Surgeon places the uterus back into its original position by reattaching pelvic ligaments or using surgical materials.
- Hysterectomy: Surgeon removes the uterus from the body through the abdomen or the vagina.
- Shirodkar sling operation:Uterine prolapse in a nulliparous
- Posterior colpoperineorrhaphy:Prolapsed pouch of Douglas
Fothergill’s operation with tubal ligation:
- Multipara with 2nd degree uterovaginal prolapse
- The Manchester operation or simply “Fothergill operation” is a technique used in gynecology operations.
- It is an operation for uterine prolapse. Its purpose is to reduce the cystourethrocele and to reposition the uterus within the pelvis.
STEPS OF FOTHERGILL-
- Preliminary dilatation and curettage
- Amputation of cervix
- strengthening the cervix by suturing cut end of Mackenrodt ligament in front of cervix
- Anterior colporrhaphy
- Posterior colpoperineorrhaphy
Indication of Manchester operation in prolapse :
- Congenital elongation of cervix
- Women of < 35 years age
- Patient who wants child bearing function
Exam Important
- Stress incontinence is a common symptom in Prolapse uterus
- Most common genital prolapse is Cystocoele
- Cause of decubitus ulcer in uterine prolapse is Venous congestion
- For Multipara with uterine prolapse the management of choice is Fothergill’s repair with tubal ligation
- Indication of Manchester operation in prolapse is Women of < 35 yrs age, Congenital elongation of cervix & Patient who wants child bearing function
- Birth trauma is a risk factor for Prolapse uterus
- Most important structure preventing uterine prolapse is Cardinal ligament
- Purandare’s cervicopexy is done in Congenital prolapse of uterus
- Pregnancy with prolapse : Pessary treatment
- Uterine prolapse in a nulliparous : Shirodkar sling operation
- Prolapsed pouch of Douglas : Posterior colpoperineorrhaphy
- Genital prolapse is best repaired after 6 months of child birth
- Fothergill’s, Ward Mayo & Le Forte operations are used for genital prolapse
- Urinary incontinence in uterovaginal prolapse is mostly is due to Stress incontience
- Treatment of choice in a multiparous female with 2nd degree uterovaginal prolapse is Fothergill’s operation with tubal ligation
- The best way to treat decubitus ulcer in a case of genital prolapse is by Reduction with tampoon
- Presence of decubitus ulcer in prolapse indicates Circulatory disturbances
- In Early pregnancy a rubber — ring passary is an appropriate management for a woman who is having utero — vaginal prolapse
- According to shaw’s classification, IIIrd degree of uterine prolapse is Cx outside the introitus
- Broad ligament doesn’t prevent prolapse of uterus
Don’t Forget to Solve all the previous Year Question asked on UTERINE PROLAPSE
Click Here to Start Quiz
Click Here to Start Quiz

