PRESSURE CURVES IN CVS
Pressure & volume changes during different phases of cardiac cycle can be represented by,
- Aortic pressure curve.
- Pressure-volume loop.
- Jugular venous pressure.
1. AORTIC PRESSURE CURVE:
Onset of rapid ejection phase of ventricular systole.
↓
Aortic pressure steeply rises to maximum.
To about 120 mm/Hg
↓
Ejection of blood into aorta → Causes aortic wall stretch → Blood in entire arterial system moves at a faster rate.
↓
Sets up pressure wave traveling along arteries, expanding their walls.
- This is palpable as “Pulse”.
Aortic pressure declines throughout diastole.
- Aortic elastic recoil property & arteriolar resistance –
– Maintains relatively high aortic pressure during diastole.
An incisura/dicrotic notch corresponds to aortic valve closure –
- Recorded in early part of downstroke of aortic pressure curve
- Produced by sudden backward flow of aortic blood.
- Followed by immediate cessation of backflow.

Pulse:
- Strength/amplitude/volume of pulse depends on,
- Stroke volume –
– Volume of blood ejected out with each beat.
- Extent of arterial wall elasticity/compliance.
- In turn both are determinants of Pulse Pressure.
2. PRESSURE-VOLUME LOOP:
- Represents “Relationship between ventricular pressure & volume throughout cardiac cycle”.
- X-axis: Presents ventricular blood volume.
- Y-axis: Presents left ventricular pressure.
- Loop width:
– Represents “Stroke volume”.
– Ie., Difference between end-diastolic volume & end-systolic volume.
- Area under loop – “Ventricular stroke work”/”External cardiac work”.
– Four phases of cardiac cycle, each representing one side of closed loop.

1. Starting with “End-diastolic volume” –
- Increased ventricular pressure.
- Volume is constant-
– Hence, isovolumetric contraction.
2. During ejection phase –
- Decreased volume.
- Pressure – Small change.
3. Isovolumetric relaxation –
- Decreased intraventricular pressure.
- Volume – No change.
4. Filling phase –
- Increased volume.
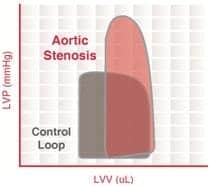
CONDITIONS SHIFTING CURVE:
LOOP SHIFTING LEFT –
- When less volume is handled by same pressure.
- Occurs in conditions with decreased compliance & increased contractility.
Eg:
- In Pressure overload – Aortic stenosis.
- In sympathetic stimulation.
- Concentric hypertrophy.
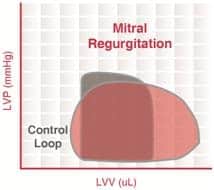
LOOP SHIFTING RIGHT-
- In volume overload – Eg. Mitral & aortic regurgitation.

3. JUGULAR VENOUS PRESSURE (JVP):
- Variations in right atrial pressure are transmitted to jugular veins producing,
– Three positive waves (a, c & v)
– Two negative waves/descents (x & y).
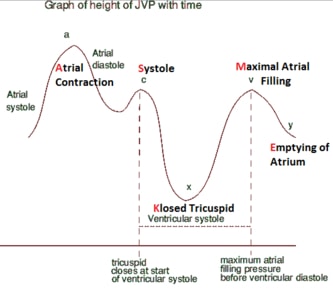
a wave –
- Presystolic ‘positive’ wave.
- Due to right atrial systole.
x-descent –
- Negative wave.
- Due to right atrial relaxation.
c-wave –
- Positive wave.
- Produced by bulging of tricuspid valve into right atrium.
- Happens during right ventricular isovolumetric contraction.
v-wave –
- Positive systolic wave.
- Due to tricuspid valve closure.
- Resulting in increased vena cava blood volume during systole.
y-descent (Diastolic collapse) –
- Negative wave.
- Due to tricuspid valve opening.
- Causing rapid blood flow into right ventricle.
Exam Important
- Aortic elastic recoil property & arteriolar resistance maintains relatively high aortic pressure during diastole.
- An incisura/dicrotic notch in an aortic pressure curve, corresponds to aortic valve closure.
- Strength/amplitude/volume of pulse depends on,
– Stroke volume – Volume of blood ejected out with each beat.
– Extent of arterial wall elasticity/compliance.
– In turn are pulse pressure determinants.
PRESSURE-VOLUME LOOP:
- Loop shifting left – Aortic stenosis.
- Loop shifting right – Mitral regurgitation & aortic regurgitation.
JUGULAR VENOUS PRESSURE (JVP):
- a wave – Due to right atrial systole.
- v-wave – During tricuspid valve closure.
Click Here to Start Quiz
