BREECH PRESENTATION
INTRODUCTION:



- In breech presentation, the lie is longitudinal and the podalic pole presents at the pelvic brim.
- Most common breech presentation is Left sacroanterior
- Breech presentation is mostly mistaken for Face presentation
- Percentage of breech at term is 3 %
VARIETIES:
Complete (Flexed breech):
- Commonly present in multiparae(10%).
- Presenting part :2 buttocks, external genitalia and two feet
Incomplete:
Breech with extended legs (Frank breech):
- Presenting part:2 buttocks and external genitalia
- Present in primigravidae(70%).
- Least chances of cord prolapse
- In breech, engagement takes places earliest in frank
Footling presentation (25%):
- Both thighs and legs are partially extended bringing the legs to present at brim.
- Knee presentation:
- Thighs are extended but the knees are flexed, bringing the knees down to present at the brim.
Clinical varieties:
- Uncomplicated:no other associated obstetric complications
- Complicated:associated with conditions which adversely influence prognosis such as prematurity, twins, contracted pelvis, placenta previa
ETIOLOGY:
- Prematurity
Factors preventing spontaneous version:
- Breech with extended legs
- Twins
- Oligohydramnios
- Septate or bicornuate uterus
- Short cord, relative or absolute
- IUD of fetus.
Favourable adaptation:
- Hydrocephalus
- Placenta previa
- Contracted pelvis
- Cornu-fundal attachment of the placenta
Undue mobility of the fetus
- Hydramnios,
- Multiparae with lax abdominal wall.
- Fetal abnormality: Trisomies 13, 18, 21, anencephaly and myotonic dystrophy
DIAGNOSIS:
Clinical:
| CHARACTERISTICS | COMPLETE BREECH | FRANK BREECH |
| Per abdomen | ||
| Fundal grip |
|
|
| Lateral grip | Fetal back is to one side & irregular limbs to other | Irregular parts are less felt on the side |
| Pelvic grip |
|
|
| FHS | Usually located at a higher level round about the umbilicus | Located at a lower level in the midline |
| Per vaginam | ||
| During pregnancy | Soft and irregular parts are felt through fornix | Hard feel of the sacrum is felt |
| During labor | Palpation of ischial tuberosities, sacrum and the feet by the sides of the buttocks | Palpation of ischial tuberosities, anal opening and sacrum only |
ULTRASONOGRAPHY:
- Detect fetal congenital abnormality
- Detect primigravidae with engaged frank breech or with tense abdominal wall and irritable uterus
- Type of breech
- It measures biparietal diameter, gestational age and estimated weight of the fetus
- Localizes the placenta
- Assessment of liquor volume
- Attitude of the head
POSITIONS:
- First position: Left sacroanterior (LSA)—being the most common
- Second position: Right sacroanterior (RSA)
- Third position: Right sacroposterior (RSP)
- Fourth position: Left sacroposterior (LSP).
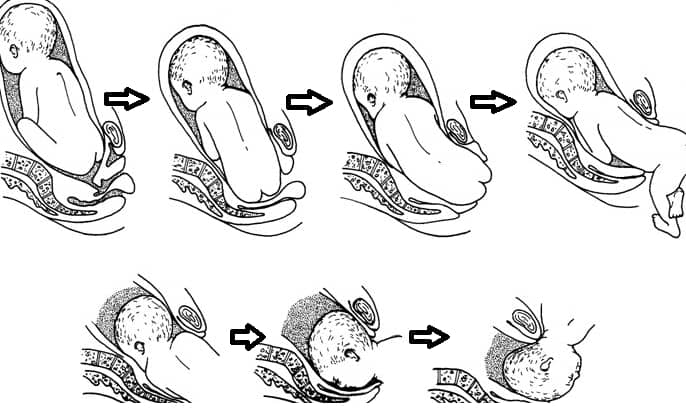
MECHANISM OF LABOR IN BREECH PRESENTATION:
SACROANTERIOR POSITION:
Principal movements occur at three places
Buttocks:
- Engaging diameter is bitrochanteric (10 cm or 4″)
- Breech is engaged when diameter passes through the pelvic brim
- Descent of the buttocks: Till anterior buttock touches the pelvic floor
- Internal rotation of the anterior buttock(1/8th of a circle)
- Further descent with lateral ! exion of the trunk
- Delivery of the trunk and the lower limbs
- Restitution
Shoulders:
- Bisacromial diameter (12 cm or 4 3/4″) engages
- Descent occurs with internal rotation of the shoulders bringing the shoulders to lie in the anteroposterior diameter of the pelvic outlet
- Ttrunk simultaneously rotates externally through 1/8th of a circle
- Delivery of the posterior shoulder followed by the anterior
- Restitution and external rotation
Head:
- Engagement:Engaging diameter of the head is suboccipitofrontal (10 cm).
- Descent with increasing # exion occurs
- Internal rotation of the occiput(anteriorly, through 1/8th or 2/8th of a circle)
- Further descent occurs until the subocciput hinges under the symphysis pubis
- Head is born by ! exion—chin, mouth, nose, forehead, vertex and occiput appearing successively.
Sacroposterior position:
- In sacroposterior position, the mechanism is not substantially modified.
- The head has to rotate through 3/8th of a circle to bring the occiput behind the symphysis pubis.
BIRTH INJURIES ASSOCIATED WITH BREECH DELIVERY COMPLICATIONS
- Brain damage
- Spinal cord injury
- Fetal distress
- Umbilical cord prolapse
- Seizures
- Cerebral palsy
- Compressed umbilical cord
- Nerve damage
- Umbilical cord wrapped around baby’s neck
- Oxygen deprivation
Exam Important
- Most common breech presentation is Left sacroanterior
- Percentage of breech at term is 3 %
- Fetal malformation , Uterine anomaly & Cornual implantation of placenta are associated with breech presentation at normal full term pregnancy
- Prematurity is the commonest cause for breech presentation
- LEAST chances of cord prolapse are seen in Frank breech
- Causes of breech presentation are Hydramnios,Septate uterus,Hydrocephalus, Placenta praevia & Pelvic contracture
- Recurrent breech presentation is seen In Congenital uterine anomaly
- Breech presentation is mostly mistaken for Face presentation
- In breech, engagement takes places earliest in frank
Don’t Forget to Solve all the previous Year Question asked on BREECH PRESENTATION
Click Here to Start Quiz
Click Here to Start Quiz
