COTRIMOXAZOLE
- Fixed drug combination of Sulfamethoxazole and Trimethoprim
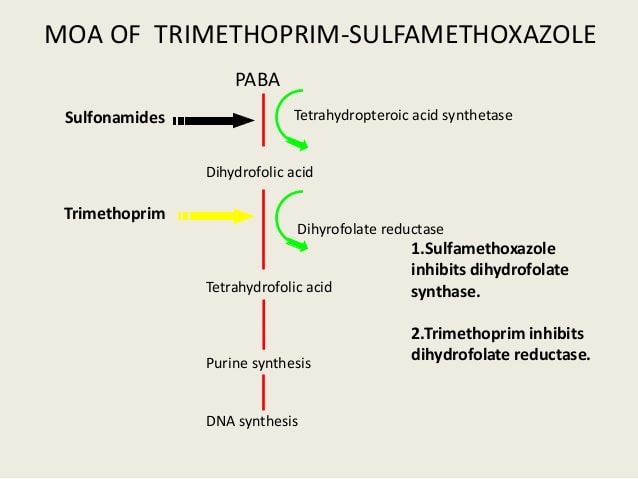
MOA:
INTRODUCTION
- Both bacteriostatic (Individually)
- Bactericidal – Combination
- Both drugs have almost similar half-lives (10 Hrs)
- Maximum synergism for sensitive organism.
- Optimal synergism obtained at 5:1 dose ratio (e.g. 800 mg:160 mg)
- TMP crosses BBB and placenta
- SMZ doesn’t cross.
- TMP – more rapidly absorbed than SMZ
- TMP – 45% plasma protein bound
- SMZ -65% bound
ANTIBACTERIAL SPECTRUM:
- Salmonella typhi, Serratia, Klebsiella Enterobacter, Yersinia & Pneumocystis jiroveci.
- Sulfonamides resistance strains of S. aureus, E. coli, gonococci, meningococci & H.influenzae.
RESISTANCE:
- Slow to develop
- By mutational changes or plasmid-mediated acquisition of DHFRase enzyme having lower affinity for inhibition.
USES:
- Uncomplicated lower urinary tract infection
- DOC grade IV vesicoureteric reflux with recurrent UTI Cotrimoxazole
- DOC for Cyclosporiasis & Isosporiasis (Protozoal infection).
- Cystitis.
- Chronic and recurrent urinary tract infections
- 3-10 days
- Respiratory tract infection –
- Lower and upper, chronic bronchitis, facio-maxillary infections, otitis media.
- Typhoid
- Bacterial diarrhoeas & dysentery: due to Campylobacter, E coli, Shigella etc.
- Pneumocystis jiroveci: Severe pneumonia – Prophylactic use in AIDS patients(CD4 count is less than 200) with neutropenia.
- Dose – DS tablet 4-6 times 2-3 weeks
- Chancroid – H. ducreyi
- Alternative to penicillin in agranulocytosis patients, septicaemia etc.
ADVERSE EFFECT:
- Nausea, vomiting, stomatitis, rash.
- Megaloblastic anaemia.
- Folate deficiency.
- Patients with marginal folate levels.
- Blood dyscrasias
- Pregnancy:
- Teratogenic risk
- Neonatal haemolysis
- Methaemoglobinaemia
- Renal disease may develop uremia
- Fever.
- Risk of bone marrow toxicity –
- Especially in elderly
- Bone marrow hyperplasia.
- Among in AIDS patients with Pneumocystis jiroveci infection.
Drug interaction:
- With diuretics – Higher incidence of thrombocytopenia
Exam Important
- Cotrimoxazole is effective against P carinii
- T/t of choice for grade IV vesicoureteric reflux with recurrent UTI Cotrimoxazole
- In cotrimoxazole, sulphamethoxazole and trimethoprim are in the ratio of-5: 1
- The drug with a definite risk of hemolysis in patients with G6PD deficiency is Cotrimoxazole
- Cotrimoxazole therapy is to be given in HIV infected patients irrespective of the presence of symptoms if the CD4 count is less than 200.
Don’t Forget to Solve all the previous Year Question asked on COTRIMOXAZOLE
Click Here to Start Quiz
Click Here to Start Quiz
