Lead poisoning
| A | Chronic lead poisoning | |
| B | Chronic mercury poisoning | |
| C | Chronic phosphorus poisoning | |
| D | Chronic gold poisoning |
| A | Chronic lead poisoning | |
| B | Chronic mercury poisoning | |
| C | Chronic phosphorus poisoning | |
| D | Chronic gold poisoning |
Chr. Lead poisoning = Plumbism = Saturnism = Saturnine poisoning– ALA in urine, Coproporphyrin in urine, facial pallor, Basophilic stippling/Punctate basophilia (dark blue, pin-head spots in cytoplasm of RBCs), Burtonian line (blue line gums’ margin, PbS, 50-70% cases, near carious/dirty teeth, Lead palsy, Pb encephalopathy, wrist drop, foot drop, Colic, Constipation, Menstrual irregularity, Sterility, Nephropathy, X-ray- radio-opaque bands at metaphyses of long bones, Pb >0.03mg% in blood is diagnostic.
Which of the following is the earliest sign of lead poisoning?
| A |
Facial pallor |
|
| B |
Colic and constipation |
|
| C |
Punctate basophilia |
|
| D |
Encephalopathy |
Facial pallor particularly of the mouth is the earliest and most consistent sign of chronic lead poisoning and is due to vasospasm.
Chronic poisoning results from a daily intake of 1-2mg of lead.
Other characteristic features of chronic lead poisoning are anaemia (punctate basophilia), lead line, colic and constipation, lead palsy and encephalopathy.
Reference:
Essentials of Forensic Medicine and Toxicology by Dr K.S Narayan Reddy 27th edition page 479.
A 25 year old plumber comes to the clinic with complaints of abdominal colic, constipation, weakness of hand and anemia since 2 years. What would be the most probable diagnosis in this patient?
| A |
Lead poisoning |
|
| B |
Gastric carcinoma |
|
| C |
Chronic pancreatitis |
|
| D |
Hookworm infestation |
The occupational history and clinical features of this patient suggest that he is suffering from chronic lead poisoning.
Characteristic features of chronic lead poisoning includes:
- Facial pallor: Particularly of the mouth is the earliest and most consistent sign.
- Anemia: Anemia associated with polychromasia, punctate basophilia, reticulocytosis, poikolocytosis, anisocytosis and sideroblastosis. Basophilic stippling refers to the presence of dark blue pin head sized spots in the cytoplasm of red blood cells.
- Lead line or Burtonian line: seen on gums in 70% cases.
- Colic and constipation seen in 85% cases.
- Lead palsy: Radial nerve is most commonly involved resuling in wrist drop.
- Encephalopathy: It is seen in every case of plumbism. Lead encephalopathy is irreversible and 85% have permanent brain damage.
| A |
At a cellular level it interacts with the sulfhydryl group |
|
| B |
Facial pallor is one of the earliest and most consistent sign |
|
| C |
Initially there may be polycythaemia |
|
| D |
None of the above |
Though lead poisoning is associated with anemia, polychromasia, punctate basophilia, reticulocytosis and increased mononuclear cells ; it may also be associated with polycythaemia and polychromatophilia in the early stages.
The facial pallor (mainly circum oral) seen in lead poisoning is believed to be due to vasospasm.
| A |
Ingestion |
|
| B |
Dermally |
|
| C |
Inhalation |
|
| D |
None of the above |
- Inhalation – Most cases of industrial lead poisoning is due to inhalation of fumes and dust of lead or its compounds.
- Ingestion – Small quantities of lead trapped in the upper respiratory tract may be ingested. Contaminated hands may also lead to ingestion.
- Skin – Only organic lead (e.g., tetraethyl lead) is absorbed dermally.
International lead poisoning prevention week is celebrated in:
| A |
January |
|
| B |
March |
|
| C |
October |
|
| D |
December |
- raise awareness about lead poisoning;
- highlight countries and partners’ efforts to prevent childhood lead poisoning; and
- urge further action to eliminate lead paint.
Protoporphyrin levels >100 μg/dl indicates:
| A |
Iron overload |
|
| B |
Lead poisoning |
|
| C |
Porphyria |
|
| D |
All of the above |
Sideroblastic anemia is caused by all except ‑
| A |
Collegen vascular disease |
|
| B |
Iron deficit |
|
| C |
Lead poisoning |
|
| D |
Cutaneous porphyria |
Ans. is ‘b’ i.e., Iron deficit
- Causes of sideroblastic anemia
Hereditary
o X-linked recessive sideroblastic anemia.
Acquired
Hematological Drugs & chemicals Others
Myelofibrosis INH RA
Myelodysplasia Penicillamine Myxedema
Acute leukemia Lead SLE
Lymphoma Alcohol Iron overload
Myeloma Pyridoxin dificiency Porphyria
Polycythemia vera Chloromphenicol
Hemolytic anemia
| A | Inhibition of enzymes involved in heme biosynthesis | |
| B |
Binding of lead to transferrin, inhibiting the transport of iron |
|
| C |
Binding of lead to cell membrane of erythroid precursors |
|
| D |
Binding of lead to ferritin inhibiting their breakdown into hemosiderin |
Ans. is ‘a’ i.e., Inhibiton of enzymes involved in Heme biosynthesis
o Lead interferes with the syntheiss of Heme by inhibiting the enzymes d Aminolevulinic acid dehydrase and Ferrochelatase. These two enzymes are involved in the synthesis of Heme.
Plumbism is caused by.
| A |
Lead poisoning |
|
| B |
Mercury poisoning |
|
| C |
Thallium poisoning |
|
| D |
Copper poisoning |
A i.e. Lead
Anaemia, punctate basophilia, constipation blue line and abdominal colic are characreristic of
| A |
Opium addiction |
|
| B |
Arsenic poisoning |
|
| C |
Mercuric poisoning |
|
| D |
Lead poisoning |
D i.e. Lead poisoning
A patient presented with encephalopathy, wrist drop, colic and constipations. Blood picture shows basophilic stippling of RBC’s. Most likely cause is :
| A |
Lead poisoning |
|
| B |
Arsenic poisoning |
|
| C |
Iron poisoning |
|
| D |
Opium poisoing |
A i.e. Lead poisoning
All are features of lead poisoning, except :
| A |
Diarrhoea |
|
| B |
Abdominal pain |
|
| C |
Encephalopathy |
|
| D |
Nephropathy |
A i.e. Diarrhoea
The earliest manifestations of Chronic lead poisoning include:
| A |
Colic and Constipation |
|
| B |
Encephalopathy |
|
| C |
Punctate basophilia |
|
| D |
Lower limb paralysis |
C i.e. Punctate basophilia
Lead poisoning is characterised by:
| A |
Diarrhoea |
|
| B |
Encephalopathy |
|
| C |
Neuropathy |
|
| D |
B and C |
Ans:D.)B and C.
CLINICAL FINDINGS of Lead Poisoning:
- The clinical findings of lead poisoning are different in the inorganic and organic lead exposures.
- Inorganic lead poisoning: Abdominal colic, constipation, loss of appetite, blue line on the gums, stippling of red cells, anemia, wrist drop and foot drop.
- Organic lead poisoning: The toxic effects of organic lead poisoning are mostly on the CNS causing insomnia, headache, mental confusion, delirium, etc.
- Characteristic features of chronic lead poisoning includes:
- Facial pallor: Particularly of the mouth is the earliest and most consistent sign.
- Anemia: Anemia associated with polychromasia, punctate basophilia, reticulocytosis, poikolocytosis, anisocytosis and sideroblastosis. Basophilic stippling refers to the presence of dark blue pin head sized spots in the cytoplasm of red blood cells.
- Saturnism = Saturnine poisoning– ALA in urine, Coproporphyrin in urine, facial pallor, Basophilic stippling/Punctate basophilia (dark blue, pin-head spots in cytoplasm of RBCs), Burtonian line (blue line gums’ margin, PbS, 50-70% cases, near carious/dirty teeth, Lead palsy, Pb encephalopathy, wrist drop, foot drop, Colic, Constipation, Menstrual irregularity, Sterility, Nephropathy, X-ray- radio-opaque bands at metaphyses of long bones, Pb >0.03mg% in blood is diagnosticLead line or Burtonian line: seen on gums in 70% cases.
- Colic and constipation seen in 85% cases.
- Lead palsy: Radial nerve is most commonly involved resuling in wrist drop.
- Encephalopathy: It is seen in every case of plumbism. Lead encephalopathy is irreversible and 85% have permanent brain damage.
| A | Abdominal colic | |
| B |
Peripheral neuropathy |
|
| C |
Anemia |
|
| D |
Encephalopathy |
B i.e. Peripheral neuropathy (Don’t get astonished this is the correct answer guys)
All the following are features of chronic lead poisoning except:
| A |
Encephalopathy |
|
| B |
Burtonian line |
|
| C |
Cutaneous blisters |
|
| D |
Constipation |
C i.e. Cutaneous blister
Which is excreted typically in lead poisoning:
| A |
Urobilinogen |
|
| B |
Coproporphyrin |
|
| C |
Bilirubin |
|
| D |
Bile salts |
B i.e. Coproporphyrin
A male came with anemia, weakness in hand and constipation since 2 years. He has abdominal pain. Most probable diagnosis is:
| A |
Lead poisoning |
|
| B |
Gastric carcinoma |
|
| C |
Chronic pancreatitis |
|
| D |
Hookworm infestation |
A i.e. Lead poisoning
Plumbism (Saturism) or chronic lead poisoning presents with Lead poisoning is indicated by
Facial pallor is the earliest sign of chronic lead poisoning (plumbism)(2. Colic pain & Constipation are most commonQ features found in about 85% of cases. Anemia & Encephalopathy are very common manifestation; minor degree of encephalopathy & anemia is seen in all most all cases. Lead palsy or Peripheral neuropathy is rather late & unconunon phenomenon seen in < 10% cases Bilsters & rain drop pigmentation is seen in chronic arsenic poisoning not lead poisoning.(2
Lead sulphide is least toxic salt of lead(2. In non exposed persons coproporphyrin (CPU) levels is <150pg/literQ
|
New |
Neuropathy (leading to weakness, wrist drop)& Nephropathy(2 =Late feature |
|
|
|
|
|
||
|
A |
Anemia with punctate basophilia (i.e. basophilic stippling)Q = Early feature |
Urine |
Blood |
|
B |
Burtonian or blue stippled lead line on gumsQ |
|
|
|
C |
Colic (abdominal pain) & ConstipationQ |
Increased levels of |
Increased levels of |
|
D |
Dry belly ache i.e. diarrhea is very rareQ |
1. Copro porphyrin |
– Lead |
|
|
Dyspepsia, Drop of wrist etc due to neuropathyQ |
(CPU)Q |
– Zinc protoporphyrin |
|
E |
EncephalopathyQ, Eosinophilia |
2. Aminolaevulinic |
– Free erythrocyte |
|
F |
Facial pallorQ (earliest sign) |
acidQ |
protoporphyrinQ |
|
Mnemonic = “New -ABCDEF” |
3. Lead |
– Basophilic stippline |
|
| A | Porphyria | |
| B |
Worm colic |
|
| C |
Lead poisoning |
|
| D |
Appendicitis |
Ans. :D.)Appendicitis.
The most common medical cause of Acute abdominal pain in children is gastroenteritis, and the most common surgical cause is appendicitis
Differential Diagnosis of Acute Abdominal Pain by Predominant Age:

| A | Encephalopathy | |
| B |
Cerebellar Ataxia |
|
| C |
Status epilepticus |
|
| D |
Peripheral neuropathy |
Ans is ‘d’ i.e., Peripheral Neuropathy
Acute lead poisoning
The most serious manifestation of lead poisoning in children is
ACUTE ENCEPHALOPATHY.
Encephalopathy includes ‑
o Persistant vomiting o Papilloedema o Lethargy o Impaired consciousness and coma
o Ataxia o Seizures o Irratibility
Peripheral Neuropathy which is common in adults is rarely seen in children except with those of sickle cell disease.
| A |
Ingestion |
|
| B |
Dermally |
|
| C |
Inhalation |
|
| D |
Through conjuctiva |
Ans. is ‘c’ i.e., Inhalation
Lead poisoning (plumbism) may occur in 3 ways : ‑
1) Inhalation – Most cases of industrial lead poisoning is due to inhalation of fumes and dust of lead or its compounds.
2) Ingestion – Small quantities of lead trapped in the upper respiratory tract may be ingested. Contaminated hands may also lead to ingestion.
3) Skin – Only organic lead (e.g., tetraethyl lead) is absorbed dermally.
September 2004
| A |
Bile |
|
| B |
Calcium |
|
| C |
Urobilinogen |
|
| D |
Coproporphyrin III |
Ans. D i.e. Coproporphyrin III
Not a symptom of inorganic chronic lead poisoning:
JIPMER 12
| A |
Constipation |
|
| B |
Insomnia |
|
| C |
Colic |
|
| D |
Anorexia |
Ans. Insomnia
Burton’s line is seen in:
Al 07; Rajasthan 11; NEET 13; JIPMER 13
| A |
Lead poisoning |
|
| B |
Arsenic poisoning |
|
| C |
Phosphorus poisoning |
|
| D |
Zinc poisoning |
Ans. Lead poisoning
Industrial worker with blue lines on gums. Most probably due to:
JIPMER 13
| A |
Arsenic poisoning |
|
| B |
Lead poisoning |
|
| C |
Mercury poisoning |
|
| D |
Copper poisoning |
Ans. Lead poisoning
In case of chronic lead poisoning, the levels of which of the following is elevated:
NIMHANS 11
| A |
Porphobilinogen |
|
| B |
6-amino levulinic acid |
|
| C |
Bilirubin |
|
| D |
Urobilinogen |
Ans. 6-amino levulinic acid
Blood examination of a worker in a welding factory shows presence of anemia and basophilic stippling. What should be suspected diagnosis ‑
| A |
Chronic Lead poisoning |
|
| B |
Mercury poisoning |
|
| C |
Copper poisoning |
|
| D |
Arsenic poisoning |
Ans. is ‘a’ i.e., Chronic Lead poisoning
The patient works in welding factory and is in continuous contact with lead. Blood examination showing anemia and basophilic stippling are consistent with lead poisoning. So the suspected diagnosis is lead poisoning.
Chronic Lead poisoning
It is characterized by :
- Facial pallor particularly around the mouth is one of the earliest and most consistent feature.
- Anemia with punctate basophilia (basophilic stippling) is also an early feature. There is reticulocytosis, poikilocytosis, anisocytosis, sideroblasts and eosinophilia.
- Burtonian line (stippled blue line) is seen on the gums on upper jaw. Similar blue line is also seen in poisoning with mercury (Hg), copper (Cu), silver (Ag), Bismuth (Bi) and iron (Fe).
- Colic (abdominal pain) and constipation (dry belly ache) : is a late manifestation.
- Encephalopathy is more in children and in poisoning with tetraethyl lead.
- Paralysis in the form of wrist and foot drop is a late manifestation, called lead palsy and is due to peripheral neuropathy. It occurs only in less than 10% of cases.
- Renovascular manifestations (nephropathy) : Hypertension, arteriolar degeneration and arteriosclerotic nephritis may occur. Rarely, lead poisoning may cause proximal tubular necrosis.
- Other features include optic atrophy, CVS and reproductive anomalies.
Investigations include :
- Blood tests : (1) > 200 punctate basophilic stippling cells per mm3 is diagnostic; (2) zinc protoporphyrin and free erythrocyte protoporphyrin > 50 mg/100 ml; and (3) increased lead and aminolaevulinic acid (> 25 mg/100 cc).
- Urine tests : (1) Increased coproporphyrin (CPU) levels, of 0.25 mg/L of lead is diagnostic.
- X-ray : (1) Radioopaque matter in GIT (if ingested within 48 hours), and (2) radioopaque lines at metaphysis oflong bones in children.
- Calcium disodium edetate is specific antidote for treatment of lead poisoning.
| A | G6PD deficiency. | |
| B |
Liver diseases. |
|
| C |
Lead poisoning. |
|
| D |
All of the above. |
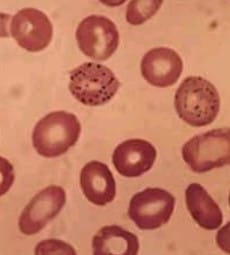
Basophilic Stippling is seen in the image.
-
Basophilic Stippling is the term used to indicate the presence of irregular basophilic granules in the cytoplasm of erythrocytes. The granules are composed of unstable RNA.
Basophilic stippling can be seen in a variety of hematologic disorders like:
-
Thalassemias
-
Heavy metal poisoning, particularly lead or arsenicals
-
Dyserythropoietic anemias
-
Megaloblastic anemia
-
Thrombotic thrombocytopenic purpura
-
Pyrimidine 5′-nucleotidase deficiency.
A young male presented with abdominal pain for the past 2 years. He also complains of weakness in his hands. His hemoblobin level was 8 gm/dL. The most likely diagnosis:
| A | Lead poisoning | |
| B |
Duodenal ulcer |
|
| C |
Carcinoma stomach |
|
| D |
Adenomatous polyposis coli |
Ans. a. Lead poisoning