Question
| A. | Immobilization in an above elbow plaster slab |
| B. |
Closed reduction |
| C. |
Plate fixation |
| D. |
Tension band wiring |

|
Correct Answer � D Explanation |
 |
Answer D) Tension band wiring
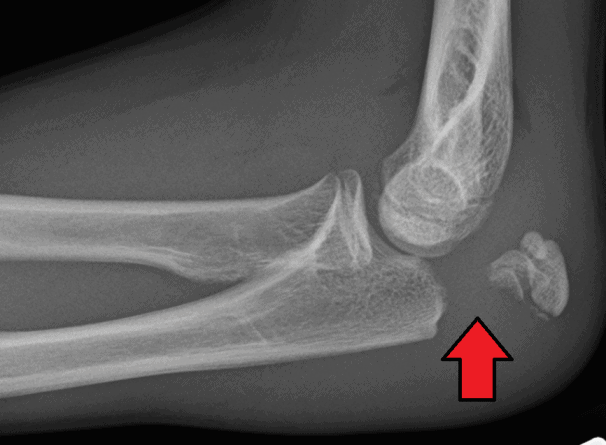
Image representsOlecranon fracture
Olecranon fracture
Olecranon fracture is a fracture of the bony portion of the elbow.
The injury is fairly common and often occurs following a fall or direct trauma to the elbow.
The olecranon is the proximal extremity of the ulna which is articulated with the humerus bone and constitutes a part of the elbow articulation.
Treatment
Nondisplaced fractures
In fractures with little or no displacement, immobilization with a posterior splint may be sufficient.
Elbows may be immobilized at 45°–90° of flexion for 3 weeks, followed by limited (90°) flexion exercises.
Displaced fractures
Most olecranon fractures are displaced and are best treated surgically:
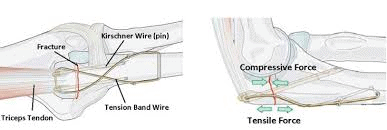
Tension band fixation
Tension band fixation is the most common form of internal fixation used for non-comminuted olecranon fractures. It is typically reserved for non comminuted fractures that are proximal to the coronoid.
This procedure is performed using Kirschner wire (K-wires) which converts tensile forces into compressive force.
Intramedullary fixation and plates
Single intramedullary screws can be used to treat simple transverse or oblique fractures.
Plates can be used for all proximal ulna fracture types including Monteggia fractures, and comminuted fractures.
Excision and triceps advancement
This method is indicated for cases when open reduction and internal fixation is unlikely to be successful.
For example: extensive comminutions, elderly patients with osteoporotic bone, and small or non-union fractures.