MULLERIAN DUCT ANOMALIES
MULLERIAN DUCTS:









- Paired ducts derived from intermediate mesoderm
- Known as paramesonephric duct.
- Mullerian ducts form as buds of coelomic epithelium .
- Grows downward & lateral to corresponding wolffian ducts.
- Turn inwards & crosses anterior to it joining its fellow from opposite side.
- Structure developing from Mullerian duct in males is Prostatic utricle
PARTS:
- Upper vertical part lateral to wolffian duct → fallopian tube.
- Middle horizontal part crossing wolffian duct → remaining part of fallopian tube.
- Lower vertical part fusing to opposite part → uterus, cervix, upper 1/3 rd of vagina.
- In forming the uterus, the mullerian ducts fuses from below upwards
MULLERIAN DUCT ANOMALY CLASSIFICATION:
In complete mullerian duct aplasia Fallopian tubes, Uterus & Vagina are likely to be absent.
46 XX karyotype
It is a seven point system that can be used to describe a number of embryonic Müllerian duct anomalies:
- class I: uterine agenesis / uterine hypoplasia
- vaginal (uterus: normal / variety of abnormal forms)
- cervical
- fundal
- tubal
- combined
- class II: unicornuate uterus/unicornis unicollis, ~15% (range 6-25%)
- communicating contralateral rudimentary horn contains endometrium
- non-communicating contralateral rudimentary horn contains endometrium
- contralateral horn has no endometrial cavity
- no horn
- class III: uterus didelphys, ~7.5% (range 5-11%)
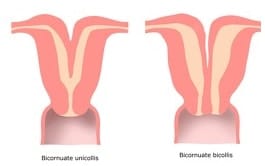
- class IV: bicornuate uterus: next commonest type, ~25% (range 10-39%)
- complete division, all the way down to the external os (bicornuate bicollis)
- partial division, not extending to the internal os (bicornuate unicollis)
- class V: septate uterus: commonest anomaly, ~45% (range 34-55%)
- complete division, all the way down to the internal or external os
- incomplete division, involving the endometrial cavity but not the cervix
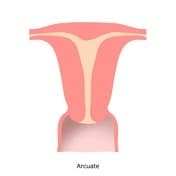
- class VI: arcuate uterus, ~7%
- class VII: in utero diethylstilbestrol (DES) exposure (T-shaped uterus)
MULLERIAN DUCT ANOMALIES CHARCTERISTICS:
- Mullerian agenesis shows Normal breast development but Fallopian tubes, Uterus & Vagina are likely to be absent
- Androgen Insensitivity Syndrome is associated
Uterine agenesis:
- Complete absence of uterine tissue above the vagina.
- Primary amenorrhoea, with normal hormonal levels guaranteed by fully functional gonads.
Unicornuate uterus:
- Second most commonly associated with miscarriages.
- Common on right side
- Associated with renal anomalies, cryptomenorrhea & primary infertility
Uterus didelphys:
- Complete duplication of uterine horns as well as duplication of the cervix, with no communication between them.
- Complete failure of mullerian duct fusion
- Mostly asymptomatic
- Dyspareunia may be seen as result of vaginal septum
Bicornuate uterus:
- Early pregnancy loss and cervical incompetence
- Incomplete fusion of paramesonephric duct
- Associated longitudinal vaginal septum, abnormal renal tract
- The most important indication for surgical repair of a Bicornuate Uterus is Habitual abortion
Septate uterus:
- Increased rate of pregnancy loss.
- Most common congenital abnormality of uterus
Arcuate uterus
- Least commonly associated with reproductive failure
T-shaped uterus:
- Most commonly associated abnormality from in utero diethylstilbestrol (DES) exposure
DIAGNOSIS:
- Unicornuate uterus: Fusiform shaped endometrial cavity tapering apex and draining into a single fallopian tube
- Uterus didelphys(IOC): 2 separate endocervical canals open into separate fusiform endometrial cavities, without communication between the two horns. Each endometrial cavity ends in a solitary fallopian tube.
- Bicornuate uterus: Divided uterus
- Septate uterus: An angle of less than 75° between the uterine horns is suggestive of a septate uterus, and an angle of more than 105° is more consistent with bicornuate uteri.
- T-shaped uterus :Opacified endometrial cavity appears small, with a shortened upper uterine segment, resulting in the characteristic T-configuration.
Other diagnostic test:
- MRI:Imaging modality of choice for septate uterus
- RADIOGRAPH
- Ultrasound:Important in Uterus didelphys & Septate uterus
Exam Important
- Complete failure of mullerian duct fusion will result in Uterus didelphys
- In complete mullerian duct aplasia Fallopian tubes, Uterus & Vagina are likely to be absent
- Mullerian agenesis shows 46 XX karyotype
- Mullerian agenesis shows Normal breast development
- The most important indication for surgical repair of a Bicornuate Uterus is Habitual abortion
- Bicornuate uterus is due to Incomplete fusion of paramesonephric duct
- MC congenital abnormality of uterus is Septate
- To diagnose uterus didelphys, procedure of choice is HSG
- Complete failure of mullerian duct fusion will result in Uterus didephys
- In cases of recurrent abortions, most common uterine malformation seen is Mullerian fusion defects
- The most important indication for surgical repair of a double uterus, such as a septate or bicornuate uterus, is Habitual abortion
- Androgen Insensitivity Syndrome condition is present with absence of both Mullerian and Wolffian duct structures
- Mullerian duct anomaly type ,Uterus didelphys is associated with the presence of two cervixes
- Normal development of ovaries in a female with absent uterus and vagina indicates Mullerian agenesis
- Mullerian fusion defects is the most common uterine malformation seen in cases of recurrent abortions
- Structure developing from Mullerian duct in males is Prostatic utricle
Don’t Forget to Solve all the previous Year Question asked on MULLERIAN DUCT ANOMALIES
Click Here to Start Quiz
Click Here to Start Quiz
