Nephrotic Syndrome
DEFINITION:
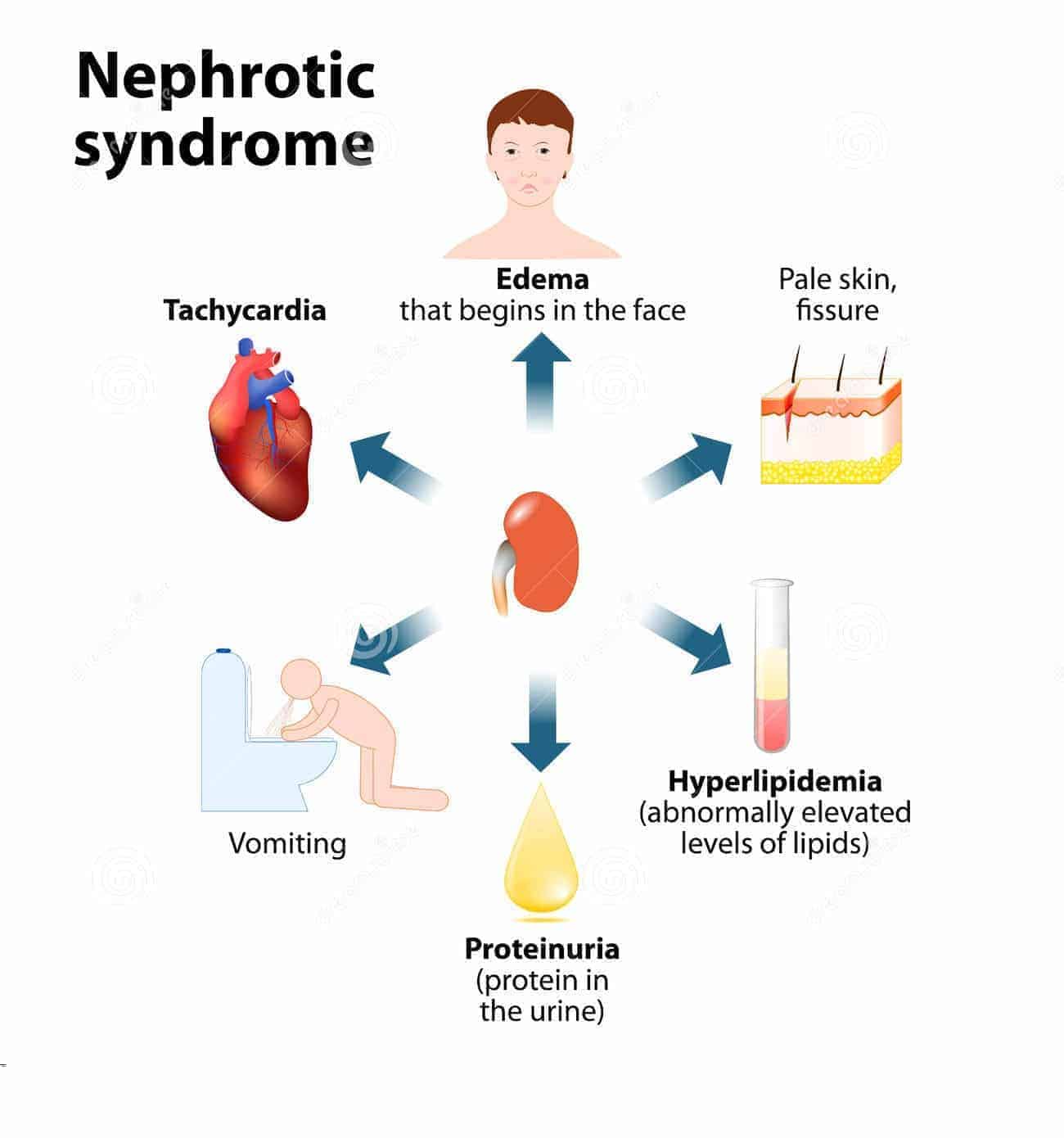
- Nephrotic syndrome is a clinical complex characterized by a number of renal and extrarenal features, most prominent of which are
- Proteinuria (in practice > 3.0 to 3.5gm/24hrs),
- Hypoalbuminemia, Edema
- Hypertension
- Hyperlipidemia, Lipiduria
- Hypercoagulabilty(result of Loss of Antithrombin III)
PATHOPHYSIOLOGY:
- Proteinuria :The glomerular structural changes damage to the endothelial surface, the glomerular basement membrane, or the podocytes..
- Hypoalbunemia : It is due to both the proteinuria and due to the increase renal catabolism (in tubules).
Infection in NS:
- Urinary immunoglobulin losses
- Edema fluid acting as a culture medium
- Protein deficiency
- Immunosuppressive therapy
- Urinary loss of a complement factor (properdin factor B) that opsonizes certain bacteria
Hyperlipedemia :
- Due to increase hepatic lipoprotein synthesis that is triggered by reduced oncotic .
- Defective lipid catabolism has also important role.
- LDL and cholesterol are increased in majority of patients whereas VLDL and triglyceride tends to rise in patients with severe disease.
Hypercoagulability :
- Increase urinary loss of antithrombin III.
- Hyperfibronogenemia due to increase hepatic synthesis.
- Increase platelet aggregability – relative immobility – haemoconcentragtion from hypovolemia – hyperlipidemia
- Hypocalcemia : Hypovolemia :Hypovolemia occurs when hypoalbuminemia decreases the plasma oncotic pressure, Resulting in a loss of plasma water into the interstitium and causing a decrease in circulating blood volume
ETIOLOGY:
Primary causes include-
- Minimal-change nephropathy(70-90% children and 10- 15%inadult)
- Focal glomerulosclerosis (15%inadult)
- Membranous nephropathy (30%inadult)
- Mesangial proliferative glomerulonephritis .
- Rapidly progressive glomerulonephritis
Secondary causes include
- Diabetes mellitus
- Lupus erythematosus
- P. malariae
- Amyloidosis and paraproteinemias
- Viral infections (eg, hepatitis B, hepatitis C, HIV )
- Preeclampsia
|
Gene |
Chromosome |
Protein |
Location |
Disease |
|
NPHS l |
19 13q |
nephrin |
slipt diaphragm |
Nephrotic syndrome of finnish type |
|
NPHS2 |
125-31(-1) |
podocin |
slit diaphragm |
Steroid resistant nephrotic syndrome |
SYMPTOMS & SIGNS:
- Anorexia
- Malaise
- Puffy eyelids
- Retinal sheen
- Edema:(due to Hypoalbuminemia) the edema is mobile – detected in the eyelids in the morning and in the ankles after ambulation
- Muehrcke lines in nails
- Focal edema may be the reason for seeking help for such complaints as: An early sign of NS is frothy urine.
- Difficulty breathing (pleural effusion or laryngeal edema),
- Substernal chest pain (pericardial effusion),
- Scrotal swelling,
- Swollen knees (hydroarthrosis),
- Swollen abdomen (ascites), and
- Abdominal pain from edema of the mesentery.
- Orthostatic hypotension and even shock may develop in children.
- Finish of nephrotic syndrome is caused by defect in Nephrin protein
- Adults may be hypo-, normo-, or hypertensive.
- Prolonged NS may result in nutritional deficiencies, including Protein malnutrition:Myopathy,
- Proteins increased in nephrotic syndrome Fibrinogen,Lipoproteins ( due to increased synthesis )
- Proteins decreased in nephrotic syndrome Albumin, Transferrin, Cholecalciferol binding protein,Thyroxin binding globulin
- Decreased total Ca++, tetany
- Spontaneous peritonitis and opportunistic infections
- Episodic hypovolemia, are a serious thrombotic risk ( renal vein thrombosis).
- Hypertension with cardiac and cerebral complications
- Hyperlipidemia and hypercholesterolemia, secondary to increased hepatic synthesis of lipoproteins and decreased clearance of lipoproteins from the circulation.
- Hyperlipidemia in these patients also cause systemic atherosclerosis.
- Marked reduction of HDL receptor protein expression also contribute to increased atherosclerosis.
DIAGNOSIS:
- Urine sediment examination
- Urinary protein measurement (24-hr)
- Serum albumin >2.5g/dl l
- Serologic studies for infection and immune abnormalities
- Renal ultrasonography
- Renal biopsy
The immunological abnormalities noted are very peculiar
- IgG antibody is decrease
- IgE and IgM antibody increase
- Reduced responses to PHA and Con A (Concanavalin A)
- Increase of beta microglobulinlevels
- Reduced production of IL 2
- Increased production of vascular permeability and immunosuppressor factors by CD4 T cells and CD 8 T cells respectively.
MANAGEMENT:
- Specific treatment
- In minimal-change nephropathy, glucocorticosteroids, such as prednisone, are used.
- Children who relapse may be treated with rituximab
- In some lupus nephritis, prednisone and cyclophosphamide are useful
- Secondary amyloidosis with nephrotic syndrome may respond to anti-inflammatory treatment of the primary disease.
- Oral cyclosporine for Steroid resistant nephrotic syndrome secondary to FSGS not responsive to methylprednisolone
- Management Acute Nephrotic Syndrome in Adults Long-Term Monitoring- Follow-up care in patients with nephrotic syndrome includes
- Diuretics will be needed; furosemide, spironolactone, and even metolazone may be used. Volume depletion may occur with diuretic use, which should be monitored.
- Anticoagulation has been advocated by some for use in preventing thromboembolic complications
- Immunization,
- Treatment of relapses of steroid-responsive nephrotic syndromes,
- Monitoring for steroid toxicity, and
- Monitoring of diuretic and angiotensin antagonist regimens.
Exam Important
- In nephrotic syndrome Transferrin, Albumin & Ceruloplasmin are reduced
- Oral cyclosporine for Steroid resistant nephrotic syndrome secondary to FSGS not responsive to methylprednisolone
- Edema in nephrotic syndrome is due to Hypoalbuminemia & Sodium and water retention
- Finnish of nephrotic syndrome is caused by defect in Nephrin protein
- The most common gene defect in idiopathic steroid resistant nephrotic syndrome NPHS 2
- Action of Tolbutamide, Diazepam & Valproate is reduced with nephrotic syndrome and hypoalbuminemia.
- Nephrotic syndrome increases the susceptibility to coronary artery disease
- Hypercoagulation in nephrotic syndrome is a result of Loss of Antithrombin III
- Muehrcke lines in nails are seen in nephrotic syndrome
- Nephrotic syndrome is the hall mark of Membranous Glomerulopathy,Minimal change disease & Focal segmental Glomerulosclerosis
- Basic abnormality in a case of nephrotic syndrome is proteinuria
- Membranoproliferative glomerulonephritis is common in both nephritic syndrome and nephrotic syndrome
- Patient with nephrotic syndrome on longstanding corticosteroid therapy may develop Hyperglycemia,Neuropsychiatric symptoms & Suppression of the pituitary adrenal axis
- Patient with congenital nephrotic syndrome requires renal biopsy
- Serum albumin level below 2.5g/dl l is seen in nephrotic syndrome in child
- Hyperglycemia ,Neuropsychiatric symptoms & Suppression of the pituitary adrenal axis are the side effects of long term steroid therapy in nephrotic syndrome
- Malaria causing nephrotic syndrome is P. malariae
- Most common cause of nephrotic syndrome in adult in Membranous glomerulonephritis
- Most common cause of nephrotic syndrome in children is Minimal change disease
- A child had hematuria and nephrotic syndrome (minimal change disease) shows Glomerular function is lost due to loss of poly charge on both sites of glomerular foot process
- Lipid cast are seen in Nephrotic syndrome
Don’t Forget to Solve all the previous Year Question asked on Nephrotic Syndrome
Click Here to Start Quiz
Click Here to Start Quiz
