Normal labour-Causes and Physiology
NORMAL LABOR (EUTOCIA):



Labor is called normal if it fulfills the following criteria.
- Spontaneous in onset and at term.
- With vertex presentation.
- Without undue prolongation.
- Natural termination with minimal aids
- Without having any complications affecting the health of the mother
CAUSES OF ONSET OF LABOR:
Uterine distension:
- By growing fetus and liquor amnii
- Increases gap junction proteins, receptors for oxytocin and specific contraction associated proteins (CAPs).
Fetoplacental contribution:
- Onset of labor→increased CRH →increased release of ACTH →fetal adrenals →increased cortisol secretion →accelerated production of estrogen and prostaglandins from the placenta
Estrogen:
- Increases release of oxytocin
- Promotes the synthesis of myometrial receptors for oxytocin, prostaglandins & increase in gap junctions in myometrial cells.
- Accelerates lysosomal disintegration
- Stimulates the synthesis of actomyosin
- Increases the excitability of the myometrial cell membranes.
Progesterone:
- Fall in level
Prostaglandins:
- Enhance gap junction formation that initiate and maintain labor
Oxytocin and myometrial oxytocin receptors:
- Receptor number increases maximum at labor
- Receptor sensitivity increases
- Oxytocin stimulate synthesis and release of PGs (E2 and F2α)
Neurological factor:
- Estrogen causes α receptors and progesterone β receptors to function
- α receptors of postganglionic nerve fibers in and around cervix, and the lower part of the uterus initiate contraction
PHYSIOLOGY OF NORMAL LABOR:
UTERINE CONTRACTION IN LABOR:
- Braxton Hicks:Painless irregular involuntary sp asmodic uterine contractions throghout pregnancy
- Waves of contractions spreads from tubal ostia downwards
- Engagement in primigravida occurs at Beginning of labour
Pattern:
- Synchronized contraction b/w both half and upper and lower part of uterus.
- Regular pattern of wave of contraction
- Fundal dominance of contractions(10–20 seconds)
- Intensity and duration higher in upper segment of uterus
- Intra-amniotic pressure rises>20 mm Hg
- Uterine blood flow Decreases
- Relaxation phase pressure
- Uterus becomes hard & pushed anteriorly
Hypogastric pain radiating to thighs due to:
- Myometrial hypoxia
- Stretching of peritoneum over fundus
- Stretching of cervix
- Stretching of uterine ligaments
- Compression of nerve ganglion
- Pain of uterine contractions is distributed along cutaneous nerve distribution of T10 to L1
- Pain of cervical dilatation and stretching is referred to back through the sacral plexus
- Maximum cervical dilatation during labor is 10 cm
Tonus:
- Intrauterine pressure in between contractions
- Quiescent:2–3 mm Hg
- First stage of labor:8 to 10 mm Hg
Intensity:Intrauterine pressure:190-300 Montevideo units
- 40–50 mm Hg in first stage
- 100–120 mm Hg in second stage
Duration:
- First stage:30 seconds
Frequency:
- First stage:at intervals of 10–15 minutes
- In second stage:every 2–3 minutes.
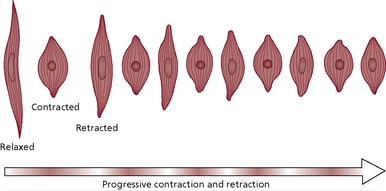
RETRACTION:
- Retraction is a phenomenon of the uterus in labor in which the muscle fibers are permanently shortened.
Effects of retraction on labor:
- Dilatation and effacement of the cervix
- Expulsion of the fetus
- Maintain the descent produced by uterine contraction
- Reduce surface area of uterus favoring separation of placenta.
- Hemostasis after separation of placenta
PRELABOR:
Lightening:
- Prior to the onset of labor due to active pulling up of the lower pole of the uterus,presenting part sinks into the true pelvis
- Incorporation of the lower uterine segment into the wall of the uterus
- Diminishes fundal height → minimizes pressure on diaphragm→relief from mechanical cardiorespiratory embarrassment
Cervical ripening:
- Soft, 80% effaced
- Due to the action of PGE2
- Admits one finger easily
- Cervical canal is dilatable.
False labor pain:
- Dull
- Confined to lower abdomen
- Relieved by enema or sedative
- Show:Expulsion of cervical mucus plug mixed with blood that represents true labour pain
Formation of “bag of waters”:
- With Dilatation of the cervical canal, lower pole of the fetal membranes becomes unsupported & tends to bulge into cervical canal.
- As it contains liquor, which has passed below the presentingpart, it is called bag of waters
- Certain sign of onset of labor
Exam Important
- Prostaglandins are the first to cause uterine contraction and lowering of blood pressure
- Braxton — Hicks contractions Occur during most of the months of pregnancy
- True labour pain is Painful uterine contraction
- Formation of the bag of waters is seen in true labour
- Progressive descent of presenting part is seen in true labour pain
- Average pressure of uterine contractions during the first stage of labour is 30 mm Hg
- Engagement in primigravida occurs at Beginning of labour
- During uterine contraction of labour, the uterine blood flow Decreases
- True labour differs from false labour by Painful uterine contractions,Progressive effacement and dilatation of the cervix & Pain often felt in front of the abdomen or radiating towards the thighs
- Pressure of normal uterine contractions is between 190-300 Montevideo units
- Bag of waters is a sure sign of labour
- Cervical ripening is mainly due to the action of PGE2
- Maximum cervical dilatation during labor is 10 cm
- True labour pains is represented by show
Don’t Forget to Solve all the previous Year Question asked on Normal labour-Causes and Physiology
Click Here to Start Quiz
Click Here to Start Quiz
