ORGANOPHOSPHATES POISONING (OPP)
INTRODUCTION:




- Organophosphate compounds are widely used in agricultural sector as PESTICIDES & as chemical war fare.
- Easily accessible, hence associated with self poisoning 200,000 /500,00 mortality associated self-poisoning with pesticides in rural Asia.
- 50-70 % in hospital based study.
- 15-30% in India
- Suicidal rate with OPC 20.6- 56.3%
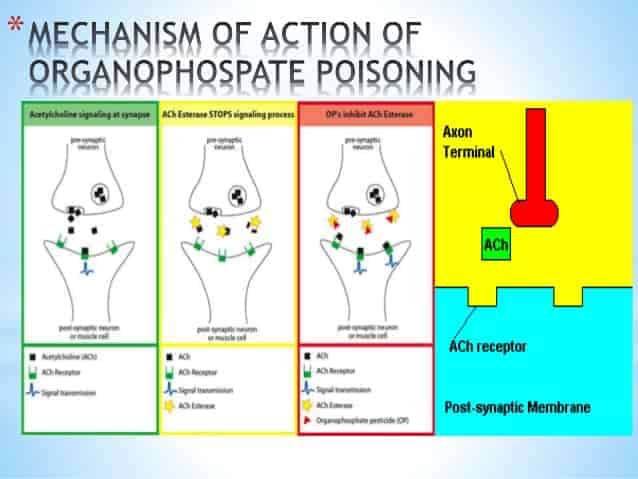
MECHANISM OF ACTION:
Irreversibly bind to serine-OH group at active site of acetylcholinesterase (AChE) & establish covalent bond (phosphorylation)
↓
AGING: loss of alkyl group + strengthening of covalent bond
↓
Phosphorylated AChE is very stable
↓
Inhibition of enzyme activity accumulation of ACh in the synapse and NMJ
↓
Overstimulation of cholinergic receptors
TYPES:
- Paralysis due to organophosphate (OP) poisoning can be three types.
1. Type I (cholinergic phase)
- Involves acute paralysis secondary to persistent depolarization at NM junction caused by persistent stimulation by excessive Ach.
- Treatment: DOC is atropine with or without oximes.
2. Type II
- Also called as “Intermediate syndrome”.
- Develops 1-4 days after resolution of acute cholinergic symptoms.
- Manifested as paralysis & respiratory distress.
- Paralysis involves proximal muscles with relative sparing of distal muscle groups.
Pathogenesis:
- Presumed to be NMJ dysfunction caused by downregulation of presynaptic & postsynaptic nicotinic receptors due to release of excessive Ach & Ca2+ respectively.
- Atropine is ineffective, symptomatic treatment is given.
3. Type III
- Involves OP-induced delayed polyneuropathy (OPIDN).
- Occurs 2-4 weeks after exposure & associated with demyelination of axons.
- Not caused by cholinesterase inhibition but rather by neuropathy target esterase (NTE) inhibition.
- Involves distal muscles with relative sparing of neck muscles, cranial nerves, & proximal muscles.
CLINICAL PRESENTATION:
Autonomic Nervous System:
- Eye: Miosis, blurred vision, pin point pupil, red tears.
- Cardiovascular: Bradycardia, hypotension.
- Glands: Extreme salivation, lacrimation, sweating.
- Gastrointestinal: Anorexia, nausea, vomiting, diarrhea.
- Respiratory: Bronchoconstriction, bronchial secretion.
- Skeletal Muscle: Fasciculations, weakness, paralysis.
- CNS: Ataxia, confusion, convulsions, coma, paralysis & tremor.
Death:
- Respiratory depression due to,
-
- Bronchoconstriction.
- Increased secretions.
- Paralysis of diaphragm & Intercostal muscles.
- Central respiratory depression.
-
MANAGEMENT OF OP:
- Diagnosis is made by Plasma cholinestrase level.
Atropine:
- Reverses muscarinic but not nicotinic
- 2 mg i.v. repeated every 10 mins till signs of full atropinization i.e dilatation of pupils ,tachycardia.
Enzyme reactivators:
- Pralidoxime (2-PAM)
- Acts by regenerating acetylcholine enzyme.
- Antidote of choice – Atrophine
Exam Important
- Muscarinic signs of OPC poisoning can be remembered as SLUDGE- BBB: Salivation, Lacrimation, Urination, Defecation, Gastric upset, Emesis, Bronchospasm, Blurred vision (Miosis), Bradycardia.
- Delayed onset polyneuropathy after organophosphorous poisoning is seen after 2-4 weeks.
- Fatality rate of organophosphorous poisoning in India is 15-30%.
- In organophosphorous compound poisoning, organophosphorous compound is a Phosphorylated enzyme irreversibly inhibit cholinesterase.
- Most specific test for organophosphorous poisoning is Plasma cholinestrase level.
- Organophosphate inhibits Esteratic site of AchEs.
- Antidote for organophosphorous poisoning is Atropine.
Don’t Forget to Solve all the previous Year Question asked on ORGANOPHOSPHATES POISONING (OPP)
Click Here to Start Quiz
Click Here to Start Quiz
