OSTEOMYELITIS
Salmonella osteomyelitis is common in
| A | Sickle cell disease | |
| B |
HIV |
|
| C | IV drug abusers | |
| D |
Pregnancy |
Salmonella osteomyelitis is common in
| A | Sickle cell disease | |
| B |
HIV |
|
| C | IV drug abusers | |
| D |
Pregnancy |
Sickle cell disease REF: Textbook of orthopedics and trauma, By GS Kulkarni, page 289
Salmonella osteomyelitis is more common in children with sickle cell disease, hemoglobinopathies and thalassemia. The reason for this higher incidence is as follows:
- Local thrombosis of intestinal mucosa causes disruption of mucosal integrity causing invasion of intra luminal bacteria
- Hyposplenmic state leads to prolongation of bacteremia to establish infection
- Hypoxia and aseptic necrosis causes multiple infarction of bone, leading to the point of low resistance favoring localization and spread of salmonella.
Commonest site of bone involvement in hematogenous osteomyelitis:
| A |
Metaphysis |
|
| B |
Diaphysis |
|
| C |
Epiphysis |
|
| D |
Point of entry of the nutrient artery |
- Acute osteomyelitis is almost invariably a disease of children. When adults are affected it may be because their resistance is lowered by debility, disease or drugs.
- Acute osteomyelitis may result from hematogenous spread of the infecting organism, or may be infected secondarily from the spread of a contiguous area of infection, or direct inoculation of bacteria in the bone (open fractures, nail punctures of the foot).
- Hematogenous spread is the commonest means of production of osteomyelitis.
- Commonest site is metaphysic. This is because of the peculiar arrangement of the blood vessels in that area, which leads to relative vascular stasis, favouring bacterial colonization.
[The nutrient artery of the long bone divides within the medullary canal of the bone, ending in small arterioles that ascend toward the growth plate. Just beneath the growth plate (physis), these arterioles twist back away from the physis and empty into venous lakes that drain into the medullary cavity. This peculiar hair-pin loop arrangement leads to relative vascular stasis and predisposes the nzetaphysis for osteomyelitis.]
- Commonest site: Lower femoral metaphyses > Upper tibial, upper femoral, upper humeral metaphyses.
- Acute hematogenous osteomyelitis behaves differently in neonates from the way it does in children. Because blood vessels cross the growth plate in neonates and infants younger than age 18 months, the bone infection that develops in that age group will likely cross the physis; however, in older children, acute infections rarely cross the growth plate.
- In adults, hematogenous infection is more common in the vertebrae than in the long bones.
Earliest site of bone involvement in hematogenous osteomyelitis:
| A |
Metaphysis |
|
| B |
Diaphysis |
|
| C |
Epiphysis |
|
| D |
Point of entry of the nutrient artery |
| A |
Streptococcus |
|
| B |
Staph aureus |
|
| C |
Corynebacterium |
|
| D |
Neisseria gonorrhoeae |
- Escherichia coli and Pseudomonas in intravenous drug users and patients with urinary tract infections.
- Haemophilus influenzae and Group B Streptococcus in neonates.
- Salmonella in patients with sickle cell disease.
Which of the following is not TRUE about osteomyelitis?
| A |
Epiphysis most commonly involved region |
|
| B |
In sickle cell anemia salmonella is causative organism |
|
| C |
Sequestrum is a piece of dead bone |
|
| D |
Involvement is dense sclerotic bone overlying a sequestrum |
Acute osteomyelitis is almost invariably a disease of children. The causative organism is usually staphylococcus aureus ( 60-80% of cases), less often streptococcus pyogenes and streptococcus pneumoniae. In children
Patients with sickle cell disease are prone to infection by salmonella.
Metaphysis is common site of osteomyelitis because of hairpin arrangements of blood vessels, Rapid growth in the region, Defective phagocytosis in the region and metaphyseal hemorrhage due to trauma in the region. The lower femoral metaphysis is commonest site for osteomyelitis.
Sequestrum is a piece of dead bone, surrounded by a infected granulation tissue.
Involucrum is a dense sclerotic bone overlying sequestrum.
Ref: Apley’s 8/e, Page 28,32; Ebnezar Textbook of Orthopedics By John Ebnezar 4/e, Page 541-42; Maheswari 3/e, Page 157-162.
Which of the following statements about tubercular osteomyelitis is not TRUE?
| A |
It is a type of secondary osteomyelitis |
|
| B |
Sequestrum is uncommon |
|
| C |
Periosteal reaction is characteristic |
|
| D |
Inflammation is minimal |
The characteristic features of tubercular osteomyelitis are soft tissue swelling and peri-articular osteoporosis.
Cystic lesions maybe seen but there is reasonably little or no periosteal reaction.
Ref: General Orthopaedics, Chapter 2, Page 70; Tuberculosis of Skeletal System By Tuli, 3rd Edition, Pages 9, 174-184; Diagnostic Musculoskeletal Imaging By Miller and Schweitzer, 2004, Page 713
A 10 year old boy is brought to the outpatient department with signs of osteomyelitis.
| A | Both Assertion and Reason are true, and Reason is the correct explanation for Assertion | |
| B |
Both Assertion and Reason are true, and Reason is not the correct explanation for Assertion |
|
| C |
Assertion is true, but Reason is false |
|
| D |
Assertion is false, but Reason is true |
Hematogenous osteomyelitis is an infection caused by bacterial seeding from the blood.
Acute hematogenous osteomyelitis is characterized by an acute infection of the bone caused by the seeding of the bacteria within the bone from a remote source. This condition primarily occurs in children. S. aureus is the most common cause of hematogenous osteomyelitis in all age groups.
| A |
Metaphysis |
|
| B |
Diaphysis |
|
| C |
Epiphysis |
|
| D |
Area around the nutrient artery |
Acute osteomyelitis:
- The metaphysis is commonly involved.
- The end vessels of the nutrient artery empty into much larger sinusoidal veins, causing a slow and turbulent flow of blood at this junction.
- Low oxygen tension in this region may compromise phagocytic activity of white blood cells.
- These conditions predispose bacteria to migrate through adjacent gaps in the endothelium and adhere to the matrix. Also,
- Staphylococcus aureus, Streptococcus, and Haemophilus influenzae are the most common causes of acute hematogenous osteomyelitis in children.
- The most common causes of septic arthritis are Neisseria gonorrhoeae, S. aureus, and group A Streptococcus.
| Staphylococcus aureus | Most common organism in osteomyelitis, acute hematogenous osteomyelitis (90%), and infected metal implants. |
| Group B strep | Infants < 1 year old |
| Haemophilus influenzae | Children 1–16 years old |
| Pseudomonas aeruginosa | Nosocomial, puncture wound through shoe |
| Pasteurella multocida | Animal bite |
| Eikenella corrodens | Human bite |
| Salmonella | Sickle cell disease |
| Anaerobes | Diabetic ulcers, fight bites |
| Candida albicans | Immunocompromised |
| Aspergillus | Immunocompromised |
| Atypical mycobacteria | Immunocompromised |
| Escherichia coli | Neonatal |
| Neisseria gonorrhoeae | Septic arthritis in young sexually active adult |
Ref: Wilson S.C., Skinner H.B. (2006). Chapter 8. Orthopedic Infections. In H.B. Skinner (Ed), CURRENT Diagnosis & Treatment in Orthopedics, 4e.
Earliest site of bone involvement in acute hematogenous osteomyelitis in children is:
| A |
Metaphysis |
|
| B |
Diaphysis |
|
| C |
Epiphysis |
|
| D |
Point of entry of the nutrient artery |
In acute hematogenous osteomyelitis in children, the metaphysis is commonly involved. The end vessels of the nutrient artery empty into much larger sinusoidal veins, causing a slow and turbulent flow of blood at this junction. These conditions predispose bacteria to migrate through adjacent gaps in the endothelium. Also, low oxygen tension in this region may compromise phagocytic activity of white blood cells. Thrombosis caused by infection results in a region of avascular necrosis that may lead to abscess formation.
- Staphylococcus aureus, Streptococcus, and Haemophilus influenzae are the most common causes of acute hematogenous osteomyelitis in children.
- The most common causes of septic arthritis are Neisseria gonorrhoeae, S. aureus, and group A Streptococcus.
| A | Both Assertion and Reason are true, and Reason is the correct explanation for Assertion | |
| B |
Both Assertion and Reason are true, and Reason is not the correct explanation for Assertion |
|
| C |
Assertion is true, but Reason is false |
|
| D |
Assertion is false, but Reason is true |
- Osteomyelitis of frontal bone results from an acute infection of frontal sinus either directly or through the venous spread.
- Pott’s puffy tumor is a complication of frontal sinusitis due to osteomyelitis of frontal bone.
- The probable diagnosis in a patient with a history of running nose and pain over the medial aspect of the eye presenting with sudden onset of high-grade fever, prostration, chemosis, proptosis and diplopia on lateral gaze with congestion of the optic disc would be Cavernous Sinus Thrombosis.
- Complications of acute sinusitis are Orbital cellulitis, Pott’s puffy tumor, and Conjunctival chemosis.
- Orbital cellulitis may occur as a complication of Parasinusitis, Faciomaxillary trauma, Endoscopic sinus surgery.
- Frontal lobe abscess may be associated with fever, papilloedema, Personality changes, and headache
Pott puffy tumor is:
| A |
Hemangiomal |
|
| B |
Osteomyelitis |
|
| C |
Osteoma |
|
| D |
None of the above |
Pott Puffy Tumor occurs if infection of frontal sinusitis spreads to the marrow of the frontal bone, causing localized osteomyelitis with bone destruction that can result in a doughy swelling of the forehead. Surgical drainage and débridement must be undertaken.
| A |
Jaw |
|
| B |
Femur |
|
| C |
Ribs |
|
| D |
Small bones of hand |
Ans. is ‘a’ i.e., Jaw
Sclerosing osteomyelitis of Garre typically develops in the jaw and is associated with extensive new bone formation that obscures much of the underlying osseous structure.
| A |
Clinical examination |
|
| B |
X-Ray |
|
| C |
CT scan |
|
| D |
MRI |
Ans. is ‘d’ i.e., MRI
- MRI is the best radiographic imaging technique for the identification of abscess and for differentiation between bone and soft tissue infection.
- MRI is the investigation of choice for the diagnosis of acute, subacute and chronic osteomyelitis with high sensitivity and specificity. The characteristic earliest signs of acute osteomyelitis include bone marrow edema, which is seen as a low T1 signal in the bone marrow, along with a high signal on T2 MRI.
- In bone:
- Cortical pathology: CT is used
- Marrow pathology: MRI is used
- Investigation of choice for avascular necrosis of bone is MRI. Since initially bone infarction occurs in the marrow.
| A |
Chronic osteomyelitis |
|
| B |
Rheumatoid arthritis |
|
| C |
Leprosy |
|
| D |
All |
Ans. Three options are correct i.e., ‘a, b & c’
Periosteal reaction in a case of acute osteomyelitis can be seen earliest at:
March 2012
| A |
5 days |
|
| B |
10 days |
|
| C |
15 days |
|
| D |
20 days |
Ans: B i.e. 10 days
The earliest sign to appear on the X-ray is a periosteal new bone deposition (periosteal reaction) at the metaphysis. It takes about 7-10 days to appear
Osteomyelitis
- Earliest site of involvement: Metaphysis
- Diagnosis of acute OM: Blood culture (positive in 65% cases)
- Periosteal reaction seen in acute OM appears after: 10 days
- MC organism in acute OM: Staph. aureus
- Brodies abscess:
– Equilibrium between host & organism;
– Abscess cavity remains without further enlargement
March 2011
| A | Streptococcus | |
| B |
Staph. aureus |
|
| C |
Salmonella |
|
| D |
H. influenza |
Ans. B: Staph. aureus
Staphylococcus aureus is the commonest causative organism causing acute osteomyelitis
Osteomyelitis:
- Earliest site of involvement in bone: Metaphysis
- Brodie’s abscess: A static cavity remains in bone, without further enlargement.
- Blood culture are positive in 65% of cases
- Periosteal reaction may be the radiological sign visible (after 10 days)
- MC cause of acute osteomyelitis: Staph. Aureus
| A | Periosteal reaction | |
| B |
Loss of plane between soft tissue and muscle |
|
| C |
Sequestrum formation |
|
| D |
Bony sclerosis |
Ans. Loss of plane between soft tissue and muscle
Earliest site of bone involvement in hematogenous osteomyelitis is ‑
| A |
Metaphysis |
|
| B |
Epiphysis |
|
| C |
Diaphysis |
|
| D |
Apophysis |
Ans. is ‘a’ i.e., Metaphysis
Pathophysiology of acute osteomyelitis
- Organism reach the bone through blood stream from a septic focus elsewhere in the body.
- Metaphysis of long bone is the earliest and most common site involved because : –
i) Metaphysis is highly vascular
ii) Commonest site is metaphysis. This is because of the peculiar arrangement of the blood vessels in that area, which leads to relative vascular stasis, favouring bacterial colonization.
[The nutrient artery of the long bone divides within the medullary canal of the bone, ending in small arterioles that ascend toward the growth plate. Just beneath the growth plate (physis), these arterioles twist back away from the physis and empty into venous lakes that drain into the medullary cavity. Thispeculiar hair-pin loop arrangement leads to relative vascular stasis and predisposes the metaphysis for osteomyelitis].
iii) Metaphysis has relatively few phagocytic cells than physis or diaphysis.
iv) Metaphysis has thin cortex.
| A | Chronic osteomyelitis | |
| B |
Acute osteomyelitis |
|
| C |
Subacute osteomyelitis |
|
| D |
Garre’s osteomyelitis |
Ans. is ‘a’ i.e., Chronic osteomyelitis
Clinical features of chronic osteomyelitis
- The commonest presenting symptom is a chronic discharging sinus. a history of bone piece discharge from the chronic sinus is considered diagnostic of chronic osteomyelitis.
- Pain is minimal or absent.
- Generalized symptoms of acute osteomyelitis are not present except in acute excacerbations.
- On examination there is irregular thickening of bone.Mi Id tenderness may be seen in deep palpation. Adjacent joint may be stiff.
Radiological features
Following are radiological features : –
- Thickening and irregularity of the cortices.
- Patchy sclerosis
- Bone cavity : This is seen as an area of rarefaction surrounded by sclerosis.
- Sequestrum(Manipal 97) : This appears denser than the surrounding normal bone because the decalcification which occurs in normal bone, does not occur in dead bone. Granulation tissue surrounding the sequestrum gives rise to a radiolucent zone around it. A sequestrum may be visible in soft tissue.
- Involucrum and cloacae may be visible.
| A | Staphylococcus aureus | |
| B |
Salmonella |
|
| C |
Pseudomonas aeruginosa |
|
| D |
Streptococcus pneumonia |
Ans. is ‘a’ i.e., Staphylococcus aureus
Acute osteomyelitis may be : –
i) Primary (hematogenous) : – Organisms reach the bone through blood stream.
ii) Secondary : – Organism gain entery directly through wound such as in compound fractures or surgical operation.
Hematogenous osteomyelitis is the commonest form of osteomyelitis and most common source of bone and joint infection is hematogenous.
It is caused most commonly by staphylococcus aureus.
Other causative organisms are streptococcus, pneumococcus, and gram negative bacilli.
Infection by pseudomonas becomes proportionally much more common in IV drug abuser. But, the most common organism is staphylococcus aureus.
| A | Staphylococcus aureus | |
| B |
Streptococcus pyogenes |
|
| C |
Mycobacterium tuberculosis |
|
| D |
Staphylococcus epidermidis |
Ans. is ‘a’ i.e., Staphylococcus aureus
Chronic osteomyelitis is nearly always a sequel to acute osteomyelitis.
Occasionally infection is subacute or chronic from the begining.
As with acute osteomyelitis, the most common causative organism is staphylococcus areus.
| A | Osteomyelitis | |
| B |
Osteochondroses |
|
| C |
Osteosclerosis |
|
| D |
Heterotopic ossification |
Ans. is ‘a’ i.e., Osteomyelitis
Ewing sarcoma is one of the differential diagnosis for subacute osteomyelitis. (see following table)
Osteomyelitis can mimic which tumor‑
| A |
Osteoclastoma |
|
| B |
Ewing sarcoma |
|
| C |
Chondroma |
|
| D |
None of above |
Ans. is ‘b’ i.e., Ewing Sarcoma
- Distinguishing between hematogenous osteomyelitis and a bone sarcoma is difficult when there is notrauma, no systemicdisease, and no sign of infection locally . Radiographic changes of soft tissue swelling, cortical tunneling, focal cancellouslysis, focal cortical resorption, and a periosteal reaction in osteomyelitis are often mistaken fbrtumors, and Ewing sarcoma is usually associated with fever
All are true about chronic osteomyelitis except ‑
| A |
Reactive new bone formation |
|
| B |
Cloaca is an opening in involucrum |
|
| C |
Involucrum is dead bone |
|
| D |
Sequestrum is hard and porus |
Pathology in chronic osteomyelitis
- Chronic osteomyelitis occurs most commonly in long bones. Bone is destroyed or devitalized in the affected part. Cavities containing pus and pieces of dead bone (sequestra) are surrounded by vascular tissue, and beyond that by areas of sclerosis due to reaction new bone formation, which may take the form of a distinct bony sheath (involucrum) Often sinus track leads to the skin surface; the sinus tends to heal and present down recurrently, but if a sequestrum is present it never heals permanently. This is because sequestra act as substrate for bacterial adhesion in much the same way as foreign implants, ensuring the persistence of infection until they are removed or discharged through perforations in the involucrum and sinuses that drain to the skin.
Sequestrum
- Sequestrum is apiece of dead bone, surrounded by infected granulation tissue trying to eat the sequestrum away.
- The sequestrum is hard, rough, porus, light in weight and lighter in colour than normal. Normal pattern of bone is lost.(Note : Sequestrum in syphilis and TB is heavier than normal bone because sclerosis usually precedes the death of the bone).
- On x-ray, sequestra show up as unnatural dense fragments, in contrast to the surrounding osteopenic bone.
Involucrum
- Involucrum is reactive new bone overlying a sequestrum.
- There may be some holes in the involucrum for pus to drain out. These holes are called cloaca.
Brodie’s abscess is ‑
| A |
Acute osteomyelitis |
|
| B |
Subacute osteomyelitis |
|
| C | Chronic osteomyelitis | |
| D |
Septic arthritis |
- Ans.C. Chronic osteomyelitis
- Brodie’s abscess is a sub-acute form of osteomyelitis, presenting as a collection of pus in bone, often with an insidious onset.
- Classically, this may present after progression to a draining abscess extending from the tibia out through the skin.
- Occasionally acute osteomyelitis may be contained to a localized area and walled off by fibrous and granulation tissue. This is termed Brodie’s abscess.
- Most frequent causative organism is Staphylococcus aureus.
- Usually occurs at the metaphysis of long bones. Distal tibia, proximal tibia, distal femur, proximal or distal fibula, and distal radius.
- Brodie’s abscess is best visualized using computed tomography (CT) scan.
- Associated atrophy of soft tissue near the site of infection and shortening of the affected bone. Osteoblastoma may be a classic sign for Brodie’s abscess.
- In the majority of cases, surgery has to be performed.
- If the cavity is small then surgical evacuation and curettage are performed under antibiotic cover.
- If the cavity is large then the abscess space may need packing with cancellous bone chips after evacuation.

| A |
Acute Osteomyelitis |
|
| B |
Subacute Osteomyelitis |
|
| C |
Chronic Osteomyelitis |
|
| D |
Tuberculous Osteomyelitis |
Ans:C.)Chronic Osteomyelitis.
Image shows:
First:Sequestrum: Large Devascularised fragment of bone separated from the healthy bone after undergoing ischemic necrosis.
Second:Involucrum: New bone deposited around a sequestrum, resulting from cortical damage stimulating the periosteum to lay down new bone, and surround the sequestrum.
Third: Brodie’s Abscess: Focal Abscess, most commonly found in metaphyses of a long bone.
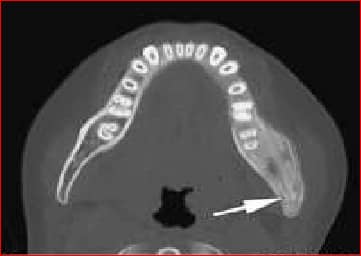
Identify this condition:

| A |
Brodies Abscess |
|
| B |
Acute Osteomyelitits |
|
| C |
Garre’s sclerosing osteomyelitis |
|
| D |
Subacute osteomyelitis |
Ans:C.)Garre’s sclerosing osteomyelitis.
Garre’s sclerosing osteomyelitis
- This is a sclerosing, non-suppurative chronic osteomyelitis.
- It is a chronic osteomyelitis with subperiosteal bone and collagen deposition.
- It may begin with acute local pain,pyrexia and swelling. Pyrexia and pain subside but the fusiform osseous enlargement persists.
- There is tenderness on deep palpation. There is no discharging sinus.
- This disease entity is well-described in dental literature and is commonly associated with an odontogenic infection resulting from dental caries
- Treatment is guarded. Acute symptoms subside with rest and broad-spectrum antibiotics. Sometimes, making a gutter or holes in the bone bring relief in pain.