PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)
PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)

- Rare acquired disorder of red cell membrane.
CAUSE & PATHOGENESIS:
- Caused due to mutations in X-linked gene “PIG-A (Phosphatidyl Inositol Glycan)”.
- This gene is responsible for Glycosyl Phosphatidyl Inositol (GPI) synthesis.
- GPI is an anchor protein which engages the Complementary Regulatory Proteins (CRP) to red cell membrane.
- Hence, mutation in PIGA gene affects CRP’s anchoring & makes RBC unduly sensitive to lytic effects of CRP.
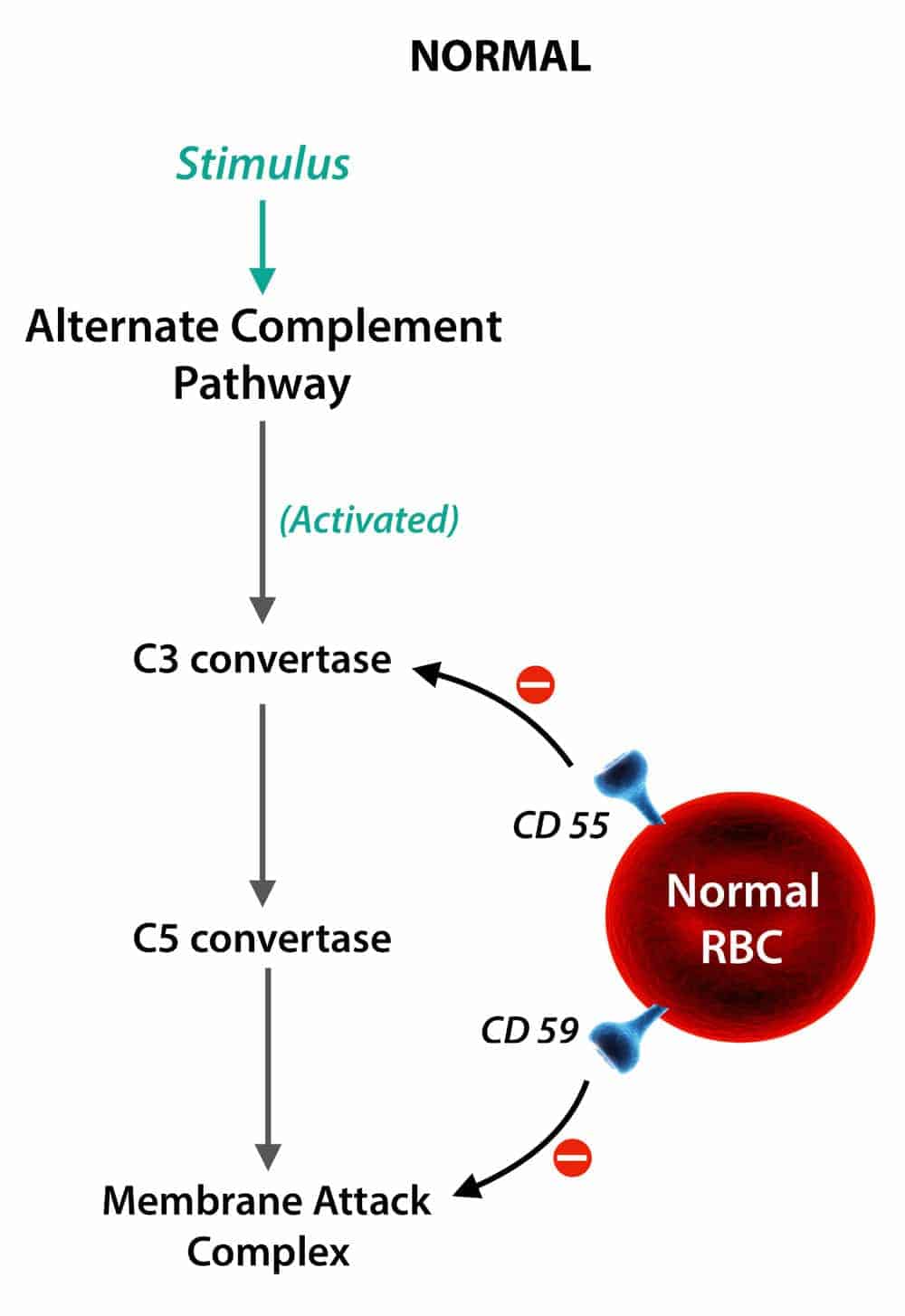
NOTE ON CRP:
- Main function of CRP – Regulates complement inactivation.
GPI defect mainly affects these 2 CRP’s:
- Membrane Inhibitor of Reactive Lysis (MIRL, CD59) – Most important protein affected.
- Decay Accelerating Factor (DAF, CD55)
CLINICAL FEATURES:
- Generally presents in adult life.
Characteristic triad includes,
1. Hemolytic anemia –
- Due to chronic intravascular hemolysis→ Causing clinical hemoglobinuria & hemosiderinuria.
- Particularly occurring as acute, intermittent & “nocturnal” hemolytic episodes.
- Identified by passage of brown urine in morning.
- Hence, referred as “Paroxysmal Nocturnal Hemoglobinuria”.
- Reduced serum ferritin levels.
- Caused due to hemosiderinuria, depleting ferritin stores.
2. Pancytopenia with hypocellular bone marrow –
- Frequently includes mild granulocytopenia & thrombo-cytopenia.
3. Venous thrombosis –
- Mainly thrombosis of hepatic veins (Budd Chiari syndrome)
- Most common cause of death in PNH.
- Cerebral & portal thrombosis also occur.
Other features:
- GPI defect affects all cells of myeloid progenitor lineage (RBCs, WBCs, platelets).
- Hence, deficient hematopoiesis & aplastic anemia.
- May develop into myelodysplastic syndrome or acute myeloid leukemia.
LABORATORY TESTS:
1. Screening:
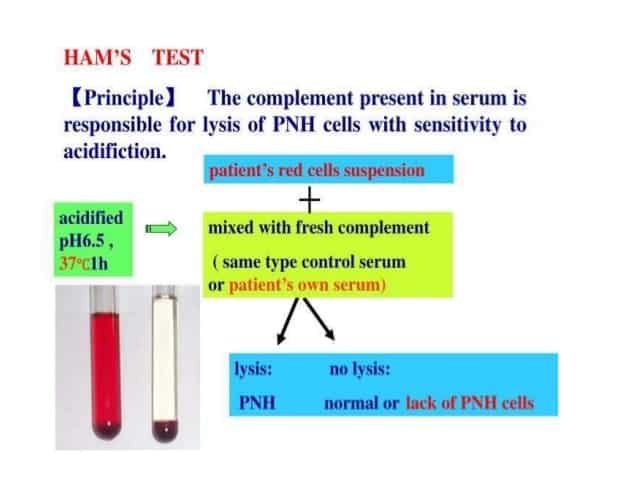
Ham’s test/(Acidified serum lysis):
- Best screening method.
- Demonstrates presence of altered sensitivity of all blood cell types (RBC, WBC & platelet) in vitro using red cell lysis at acidic pH.
- Sucrose hemolysis test.
2. Confirmatory:
Flow cytometry

- Used to detect CRP’s (CD59, MIRL) & (CD55, DAF).
- Absence or reduced expression of CD55 & CD59 on RBC membrane is diagnostic.
TREATMENT:
Eculizumab
- An anti-C5 monoclonal antibody.
- By blocking complement cascade downstream of C5, eculizumab abrogates complement-dependent intravascular hemolysis in all PNH patients.
Exam Important
- PNH caused due to mutations in “PIG-A” (Phosphatidyl Inositol Glycan) gene.
- PIGA gene is responsible for biosynthesis of Glycosyl Phosphatidyl Inositol (GPI).
- Mutation in PIGA gene causes defective production of GPI resulting in undue to sensitivity of RBC’s to CRP.
- A stem cell disorder affecting all the three cell lines (RBCs, leucocytes & platelets) is PNH.
- Flow cytometry is the confirmatory test for PNH.
- Hams test is the best screening test for PNH.
- Eculizumab, an anti-C5 monoclonal antibody is used for treating PNH.
- PNH presents with chronic hemolytic anemia, pancytopenia with hypocellular marrow & venous thrombosis.
- Venous thrombosis of hepatic veins is main cause of death in PNH – Budd Chiari syndrome.
- Reduces serum ferritin levels noted, due to hemoglobinuria & hemosiderinuria.
- Main CRP mutated is Membrane Inhibitor of Reactive Lysis (MIRL, CD59).
- PNH is associated with a decreased leukocyte alkaline phosphate scape.
Don’t Forget to Solve all the previous Year Question asked on PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)
Click Here to Start Quiz
Click Here to Start Quiz
