ROLE OF USG IN OBSTETRICS
Transvaginal USG can detect fetal cardiac activity in:
| A | 6 weeks | |
| B | 7 weeks | |
| C |
8 weeks |
|
| D |
10 weeks |
Transvaginal USG can detect fetal cardiac activity in:
| A |
6 weeks |
|
| B |
7 weeks |
|
| C |
8 weeks |
|
| D |
10 weeks |
Ans. is a i.e. 6 weeks
Embryonic investigations suggest that cardiac contractions begin in fetus at 36 days gestational age.° This is evident on : Transvaginal USG
At 6 weeks of gestational age corresponding to 13 – 18mm of MSD Transabdominal USG At 8 weeks of gestational age corresponding to 25 mm of MSD.
Note : MSD is mean Sac diameter
According to Williams Obs 23/e p 200 Using real time sunography with a vaginal transducer fetal cardiac activity ‘–‘?0 hs seen as early as 5th menstrual week
| A | Gestation sac | |
| B |
Fetal node |
|
| C |
FSH |
|
| D |
Fetal skeleton |
Ans. is a i.e. Gestational sac
“The first definitive sonographic finding to suggest pregnancy is visualization of the gestational sac.” First sign of intrauterine pregnancy is presence of yolk sac within the gestational sac.°
Extra Edge
- The position of a normal gestational sac is in the mid to upper uterus.
- As the sac implants into the decidualized endometrium it is adjacent to the linear central cavity echo complex without displacing this echogenic anatomic landmark. This is known as Intradecidual Sign.
- As the sac enlarges it gradually impresses on and deforms the central cavity echo complex giving rise to the characteristic sonographic appearance of the double decidual sac sign°
This sign is most effective with transabdominal sonography, performed at 5 – 6 weeks gestational age because using this approach, sonographer can confirm the presence of an intrauterine pregnancy before a yolk sac is identified.
Study of fetal parts in first trimester with least radiation hazard :
| A | X-ray abdomen | |
| B |
Pelvimetry |
|
| C |
CT scan |
|
| D |
Ultrasound |
Ultrasound
USG can detect gestation sac earliest at:
| A |
5-6 weeks of gestation |
|
| B |
7-8 weeks of gestation |
|
| C |
10 weeks of gestation |
|
| D |
12 weeks of gestation |
A i.e. 5-6 weeks of gestation
All are signs /features of ectopic pregnancy on USG except
| A |
Pseudo sac |
|
| B |
Hyprechoic ring |
|
| C |
Adenexal mass |
|
| D |
Echogenic mass with multicystic spaces within endometrial cavity |
D i.e. Echogenic mass with multicystic spaces within endometrial cavity
Ectopic pregnacny, characteristic finding in USG is:
| A |
Absence of gestational sac in uterus |
|
| B |
Complex adenexal mass |
|
| C |
Resistance in coloured Doppler |
|
| D |
Free fluid in peritoneal cavity |
A i.e. Absence of gestational sac in uterus
Best method of diagnosing unruptured ectopic pregnancy is combination of transvaginal sonography & quantitative B-HCG valuesQ.
Most accurate assessment of gestational age by USG is done by
| A |
Femur length |
|
| B |
Gestational sac size |
|
| C |
Menstrual history |
|
| D |
Crown rump length |
D i.e. Crown rump length
Investigation of choice in diabetic mother with a doubtful abnormal fetus:
March 2004
| A | USG | |
| B |
Glycosylated hemoglobin |
|
| C |
Amniocentesis |
|
| D |
Chorionic villous biopsy |
Ans. A i.e. USG
Accurate diagnosis of anencephaly on ultrasound can be done at:
September 2005
| A |
5 weeks of gestation |
|
| B |
8 weeks of gestation |
|
| C |
10 weeks of gestation |
|
| D |
14 weeks of gestation |
Ans. C: 10 weeks of gestation
In the first half of the pregnancy, the diagnosis is made by the elevated alfa-fetoprotein in amniotic fluid and confirmed by sonography.
The findings at 13 weeks are:
- Absence of cranial vault
- Angiomatous brain tissue
In the later half of the pregnancy the diagnosis is difficult specially when associated with hydramnios.
| A | Multiple pregnancy | |
| B |
Fetal anomalies |
|
| C |
To estimate gestational age |
|
| D |
To know the position of the placenta |
Ans. D: To know the position of the placenta
Benefits of the first-trimester USG:
- Viability of the fetus
- Pregnancy dating
- Multiple pregnancy detection
- Detection of ectopic pregnancy
- Detection of H.Mole
- Detection of fetal anomalies
Placental localization can be done with USG in the second half of pregnancy.
| A |
Hydrops fetalis |
|
| B |
Cystic hygroma |
|
| C |
Anencephaly |
|
| D |
All of the above |
Ans. D: All of the above
Common anomalies that can be seen in USG are:
- Cranial anomalies-anencephaly, hydrocephalus.choroid plexus cysts
- Cystic Hygroma
- Spinal anomalies-Spina Bifida occult and Spina bifida aperta
- Fetal heart
- Fetal abdomen and abdominal wall-Esophageal atresia, omphalocele, gastroschisis
- Hydrops fetalis
September 2009
| A |
Duodenal atresia |
|
| B |
Fetal hydrops |
|
| C |
Down’s syndrome |
|
| D |
Anencephaly |
Ans. D: Anencephaly
Common examples include hydrocephalus, anencephaly, myelomeningocoele, achondroplasia and other dwarfism, spina bifida, exomphalos, Gastroschisis, duodenal atresia and fetal hydrops.
First trimester ultrasonic ‘soft’ markers for chromosomal abnormalities such as the absence of fetal nasal bone, an increased fetal nuchal translucency (the area at the back of the neck) are now in common use to enable detection of Down syndrome fetuses.
Ultrasound can also assist in other diagnostic procedures in prenatal diagnosis such as amniocentesis, chorionic villus sampling, cordocentesis (percutaneous umbilical blood sampling) and in fetal therapy.
| A | 6-12 weeks of pregnancy | |
| B |
13-19 weeks of pregnancy |
|
| C |
20-26 weeks of pregnancy |
|
| D |
27-32 weeks of pregnancy |
Ans. is A. i.e. 6-12 weeks of pregnancy
By 10 weeks of gestational age, the fetal cranium, brain, neck, trunk, and extremities can be visualized and gross anomalies can be detected in the first trimester (abnormalities excluding nuchal translucency).
The earliest anomaly to be detected on USG: Anencephaly
Anencephaly can be detected earliest by 10 weeks. For the best diagnosis of anencephaly, USG should be done at 14 weeks.
Embryonic structure, identified earliest on USG, for confirmation of pregnancy is:
| A |
Fetal pole |
|
| B |
Fetal Heart activity |
|
| C |
Gestation sac |
|
| D |
Fetal skeleton |
Ans. C: Gestation sac
- Gestation sac and embryonic yolk sac is identified at menstrual age of 5 weeks.
- Fetal pole and cardiac activity are identified on USG at menstrual age of 6 weeks.
- Lower limb buds, upper limb buds and spine at 7, 8 and 9 weeks respectively.
Important:
- The total duration of pregnancy: 280 days
- Earliest detection of pregnancy by USG: Gestational sac
- Transvaginal sonography detects gestational sac: at 14 days after ovulation.
Pregnancy is confirmed by:
1. Fetal heart rate
2. Fetal sac on USG
3. Fetal movements
Best time to do USG in pregnancy, if it is to be done once in entire pregnancy, would be:
| A |
6-8 weeks |
|
| B |
10-12 weeks |
|
| C |
18-22 weeks |
|
| D |
34-36 weeks |
Ans. C: 18-22 weeks
Routine USG at 18-22 weeks gestation has the following effects
1) Reduces the incidence of post-term pregnancy (39%) and rates of induction of labor for post-term pregnancy.
2) Increases early detection of multi-fetal pregnancy (92%).
3) Increases early detection of major fetal anomalies when termination is possible.
4) No significant differences in clinical outcomes such as perinatal mortality.
5) Reduces neonatal admission to the special care baby unit (14%).
Best parameter by USG to assess fetal maturity:
| A |
Crown rump length at 16 weeks |
|
| B |
Head circumference at 36 weeks |
|
| C |
Biparietel diameter at 12 weeks |
|
| D |
Femur length at 12 weeks |
Ans. Biparietel diameter at 12 weeks
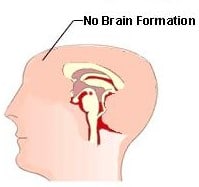
The condition shown in the image below can be diagnosed by USG as early at which week of gestation?
| A |
5 weeks of gestation. |
|
| B |
8 weeks of gestation. |
|
| C |
10 weeks of gestation. |
|
| D |
14 weeks of gestation. |
Ans:C-10 weeks of gestation.
The condition shown in the picture above represents anencephaly.
Anencephaly
- It is characterized by the absence of the cranial vault and cerebral hemispheres.
- It is the most common type of neural tube defect.
- Occurs when the rostral (head) end of the neural tube fails to close, usually between the 23rd and 26th day following conception
- Anencephaly may be sonographically detectable as early as 10 weeks.
- Ultrasound has an accuracy of approximating 100% at 14 weeks
- Features seen are:
- no parenchymal tissue is seen above the orbits and calvarium is absent: parts of the occipital bone and midbrain may be present
- less than expected value for the crown-rump length (CRL)
- a “frog eye” or “mickey mouse” appearance may be seen when seen in the coronal plane due to absent cranial bone/brain and bulging orbits.
- may show evidence of polyhydramnios: due to impaired swallowing
Typical appearance of Uterus on USG Photograph is seen in

| A |
Menstruation |
|
| B |
Hydatiform mole |
|
| C |
Twin pregnancy |
|
| D |
Acute hydramnios |
Hydatiform mole (Appearance shown: Snow storm appearance)
Molar pregnancy is an abnormal form of pregnancy in which a non-viable fertilized egg implants in the uterus and will fail to come to term. A molar pregnancy is a gestational trophoblastic disease which grows into a mass in the uterus that has swollen chorionic villi. These villi grow in clusters that resemble grapes. A molar pregnancy can develop when a fertilized egg does not contain an original maternal nucleus. The products of conception may or may not contain fetal tissue. It is characterized by the presence of a hydatidiform mole (or hydatid mole, mola hydatidosa). Molar pregnancies are categorized as partial moles or complete moles, with the word mole being used to denote simply a clump of growing tissue, or a growth.
First trimester USG finding in Down syndrome‑
| A |
Nuchal thickening |
|
| B |
Nuchal translucency |
|
| C |
Cardiac anomalies |
|
| D |
GI anomalies |
Ans. is ‘b’ i.e., Nuchal translucency