Tympanic Membrane
| A | Anterior superior quadrant | |
| B |
Anterior inferior quadrant |
|
| C |
Posterior superior quadrant |
|
| D |
Posterior inferior quadrant |
Most common site of perforation of tympanic membrane in ASOM is
| A |
Anterior superior quadrant |
|
| B |
Anterior inferior quadrant |
|
| C |
Posterior superior quadrant |
|
| D |
Posterior inferior quadrant |
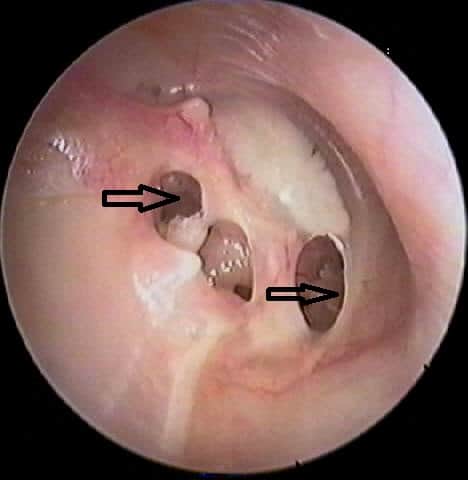
A patient presented with the following picture of Tympanic Membrane. Most Probable diagnosis (marked with arrow)
| A |
Tubercular Otitis Media |
|
| B |
Syphilitic Otitis Media |
|
| C |
Pseudomonas infection |
|
| D |
Fungal Otitis Media |
Tympanic membrane showing multiple perforations
- Infection reaches the middle ear through eustachian tube.
- The rare modes of infection are through hematogenous spread from tubercular focus in lung, tonsils, cervical lymph nodes; or due to ingestion of infected cow’s milk.
- It usually affects children and young adults.
| A |
120 dB |
|
| B |
160 dB |
|
| C |
90 dB |
|
| D |
80 dB |
Ans. B 160 Ref: Park; 22nd edi, pg –668
Deafness is the most serious pathological effect of noise. Temporary hearing loss occur in frequency range between 4000 and 6000 Hz.
Repeated or continuous exposure to noise around 100 decibels may result in a permanent hearing loss.
Non-auditory effects include interference with speech, annoyance, reduction in efficiency, and psychological changes such as rise in BP, rise in intracranial pressure, an increase in heart rate, breathing and sweating.
Exposure to noise above 160 dB may rupture the tympanic membrane and cause permanent loss of hearing.
Use of nitrous oxide is contraindicated in all of the following surgeries, EXCEPT:
| A |
Tympanic membrane grafting |
|
| B |
Pneumoencephalography |
|
| C |
Vitreoretinal surgery |
|
| D |
Exenteration operation |
Conditions in which nitrous oxide might be hazardous include,
- Air embolism
- Pneumothorax
- Acute intestinal obstruction
- Intracranial air (tension pneumocephalus following dural closure or pneumoencephalography)
- Pulmonary air cysts
- Intraocular air bubbles
- Tympanic membrane grafting
Ref: Morgan, Jr. G.E., Mikhail M.S., Murray M.J. (2006). Chapter 7. Inhalation Anesthetics. In G.E. Morgan, Jr., M.S. Mikhail, M.J. Murray (Eds), Clinical Anesthesiology, 4e.
The torture method involving simultaneous beating of both ears with palms of hand, resulting in rupture of tympanic membrane is called?
| A |
Falanga |
|
| B |
Waterboarding |
|
| C |
Telefono |
|
| D |
Dunking |
Falanga involves beating on sole of feet. In dunking the victim is immersed in water.
In water boarding the victim is immobilised in a supine position with head inclined downwards and water is poured on the face.
| A |
Magnification |
|
| B |
Removal of foreign body from the ear |
|
| C |
As applicator for the powdered antibiotic of ear |
|
| D |
Assessment of movement of the tympanic membrane |
Siegel’s speculum has an eyepiece, which is a convex lens with a magnification of 2.5 times. The eyepiece is connected to an aural speculum. It is not used to remove foreign body from the ear.
Indications: It is used to provide a magnified view of ear drum, to test mobility of ear drum by varying the pressure of external canal, to suck out middle ear secretions in patients with chronic serous ottitis media and to instill ear drops into the middle ear.
Ref: Clinical Examination Techniques in Otology 2012 By Balasubramanian, Section 5; Essentials of Otolaryngology By Frank E. Lucente, 5th Edition, Page 121
A young man presents with an accident leading to loss of hearing in the right ear. On otoscopic examination, the tympanic membrane was intact. Pure tone audiometry shows an Air – Bone gap of 55 dB in the right ear with normal cochlear reserve. Which of the following will be the likely tympanometry finding?
| A |
As type tympanogram |
|
| B |
Ad type tympanogram |
|
| C |
B type tympanogram |
|
| D |
C type tympanogram |
The threshold of bone conduction is a measure of cochlear function in pure tone audiometry.
The difference in the thresholds of air and bone conduction (A-B) is a measure of the degree of conductive deafness.
Here this patient is having a normal cochlear function.
So A-B gap of 55 dB will be because of defect in air conduction.
Otoscopic examination showed an intact tympanic membrane means the ossicular discontinuity will be the reason for the hearing loss.
| A |
Gentamicin |
|
| B |
Hearing aid |
|
| C |
Stapedectomy |
|
| D |
Sodium fluoride |
Which of the following conditions is associated with maximum hearing loss?
| A |
Otitis media with effusion |
|
| B |
Partial fixation of the stapes footplate |
|
| C |
Ossicular disruption with intact tympanic membrane |
|
| D |
Disruption of malleus and incus as well tympanic membrane |
Maximum hearing loss occurs when there is an ossicular interruption with intact tympanic membrane (54dB).
Ossicular interruption with perforation results in 38dB hearing loss, hearing loss in otitis media with effusion averages about 26-30 dB.
Partial or complete fixation of the stapes results in conductive hearing loss that ranges from 5dB to 60dB.
| A |
Both Assertion and Reason are true, and Reason is the correct explanation for Assertion |
|
| B |
Both Assertion and Reason are true, and Reason is not the correct explanation for Assertion |
|
| C |
Assertion is true, but Reason is false |
|
| D |
Assertion is false, but Reason is true |
Longitudinal fractures cause conductive hearing loss. They are the most common fractures of the temporal bone. This fracture typically results from a direct blow to the temporal or parietal aspects of the head. Symptoms at presentation include conductive hearing loss, bloody otorrhea, and loss of consciousness. Fractures extending through the mastoid rather than ear canal can result in hemotympanum without laceration of the tympanic membrane.
A middle aged female presented with complaints of progressive deafness and tinnitus. On examination, deafness is conductive in nature. Otoscopy shows a red reflex through intact tympanic membrane. “Pulsation sign” is positive.
| A | Both Assertion and Reason are true, and Reason is the correct explanation for Assertion | |
| B |
Both Assertion and Reason are true, and Reason is not the correct explanation for Assertion |
|
| C |
Assertion is true, but Reason is false |
|
| D |
Assertion is false, but Reason is true |
- Glomus tumors are benign, exquisitely painful tumors arising from specialized smooth muscle cells of glomus bodies, arteriovenous structures involved in thermoregulation.
- It is found in the dome of the jugular bulb or on the promontory along the course of the tympanic branch of the IXth cranial nerve.
- Although they may superficially resemble cavernous hemangiomas, glomangiomas arise from smooth muscle cells, rather than endothelial cells.
- They are most commonly are found in the distal portion of the digits, especially under the fingernails. Excision is curative.
-
Microscopically, the tumor cells containing neurosecretory granules are arranged in typical organoid pattern or nests. The tumor may extend locally to involve the skull and brain but may rarely metastasize.
| A |
Complete obstruction of ear canal |
|
| B |
Perforation of tympanic membrane |
|
| C |
Ossicular interruption with intact tympanic membrane |
|
| D |
Ossicular interruption with perforation |
Average hearing loss in different lesions:
- Complete obstruction of ear canal = 30db
- Perforation of tympanic membrane = 10-40 db
- Ossicular interruption with intact tympanic membrane= 54db
- Ossicular interruption with perforation = 38db
- Closure of oval window can cause 60 db hearing loss
| A |
Air conduction equals bone conduction in his left ear |
|
| B |
Air conduction equals bone conduction in his right ear |
|
| C |
Air conduction is greater than bone conduction in his right ear |
|
| D |
Bone conduction is greater than air conduction in his left ear |
This patient has sensorineural deafness in his right ear due to his acoustic neuroma. In the normal ear, air conduction is greater than bone conduction. An ear with sensorineural deafness will still have air conduction greater than bone conduction, however both will be qualitatively decreased.
| A |
Anterior superior quadrant |
|
| B |
Anterior inferior quadrant |
|
| C |
Posterior superior quadrant |
|
| D |
Posterior inferior quadrant |
In acute suppurative otitis media, 85% of cases show a small perforation in antero-inferior quadrant of pars tensa.
Perforations in this location were associated with smooth margins, good drainage of pus, and a favorable clinical course.
Hence this area is termed as “perforation zone”.
Only 15% of perforations occurred in other locations, most typically the posterior-superior quadrant.
Which structure is attached to the center of the tympanic membrane?
| A |
Footplate of the stapes |
|
| B |
Handle of the malleus |
|
| C |
Long process of the incus |
|
| D |
Tragus |
A man presented with pulsatile tinnitus and hearing loss. A vascular mass is seen behind the tympanic membrane. Diagnosis can be:
| A |
Glomus Jugulare |
|
| B |
Ca mastoid |
|
| C |
Acoustic neuroma |
|
| D |
Angiofibroma |
Tympanogram of a 70 year old male with hearing loss and tinnitus revealed a type B wave. On examination he has a conductive type of deafness and a dull tympanic membrane on the right side. Lympadenopathy was present in the posterior triangle of neck. The most likely diagnosis is:
| A |
Middle ear tumor |
|
| B |
Nasopharyngeal malignancy |
|
| C |
Acoustic neuroma |
|
| D |
T.B of middle ear |
The presence of conductive type of hearing loss, dull tympanic membrane and type B tympanogram suggests the presence of middle ear cavity or serous otitis media.
Serous otitis media in an older individual should raise the suspicion of nasopharyngeal malignancy. The presence of enlarged lymph nodes adds to the suspicion.
The following structure represents all the 3 components of the embryonic disc-
| A |
Tympanic membrane |
|
| B |
Retina |
|
| C |
Meninges |
|
| D |
None of the above |
A i.e. Tympanic membrane
Tympanic membrane derived from first pharyngeal membrane (which seperates 1st pharyngeal groove from 1st pharyngeal pouch) represents all three layers of embryonic disco. It develops from three sources. 1) External very thin skin is derived from ectoderm of 1st pharyngeal groove; 2) Medoderm of 1st & 2hd pharyngeal arches; 3) Internal lining is derived from endoderm of tubotympanic recess, (a derivative of 1st pharyngeal pouch).
| A |
Auriculotemporal |
|
| B |
Lesser occipital |
|
| C |
Greater occipital |
|
| D |
Parasympathetic ganglion |
A i.e. Aurico-temporal nerve
The treatment of traumatic rupture of tympanic membrane is-
| A |
Aural packing |
|
| B |
Chloromycetin ear dorps |
|
| C |
Tympanoplasty |
|
| D |
No active treatment |
Ans. is ‘d’ i.e., No active treatment
T/T of traumatic rupture of tympanic membrane.
- Systemic antibiotics and topical optic medications are not required unless suppurative otorrhoea is present.
- Close follow up examination is necessary to ensure that Spontaneous healing occurs.
- If the tympanic membrane does not heal within several months, surgical graft repair should be considered.
| A |
Extradural hemorrhage |
|
| B |
Subdural hemorrhage |
|
| C |
Intraventricular hemorrhage |
|
| D |
Basilar fracture |
Ans. is ‘d’ i.e. basilar fracture
What is the color of the normal tympanic membrane?
| A |
Pearly white |
|
| B |
Gray |
|
| C |
Yellow |
|
| D |
Red |
The most mobile part of the tympanic membrane:
| A |
Central |
|
| B |
Peripheral |
|
| C |
Both |
|
| D |
None of the above |
Pars flaccida of the tympanic membrane is also called
| A |
Reissner’s membrane |
|
| B |
Shrapnell’s membrane |
|
| C |
Basilar membrane |
|
| D |
Secondary tympanic membrane |
Situated above the lateral process of malleus between the notch of Rivinus and the anterior and posterior malleal folds.
- Reissner’s membrane – Separates scala media from scala vestibuli in the inner ear
- Basilar membrane – Seen in scala media and supports the organ of corti
- Secondary Tympanic Membrane – Closes the scala tympani at the site of round window
| A | 3 mm | |
| B |
4 mm |
|
| C |
6mm |
|
| D |
2 mm |
The distance of promontory from tympanic membrane:
| A |
2 mm |
|
| B |
5 mm |
|
| C |
6 mm |
|
| D |
7 mm |
“When seen in coronal section, the cavity of the middle ear is biconcave, as the medial and lateral walls are closest to each other in the center.”
The distances separating them are:-
- Near the roof 6 mm in the epitympanum (Attic)
- In the centre 2 mm in the mesotympanum
- Near the floor 4 mm in the hypotympanum
The medial wall of the tympanic cavity is formed by the labyrinth and the lateral wall is formed by the tympanic membrane.
| A |
55 mm2 |
|
| B |
70 mm2 |
|
| C |
80 mm2 |
|
| D |
90 mm2 |
The effective diameter of the tympanic membrane:
| A |
25 mm2 |
|
| B |
30 mm2 |
|
| C |
40 mm2 |
|
| D |
45 mm2 |
Area of tympanic membrane is 90 mm2.
Effective area is 55 mrn2(approximately 2/3 of the total area).
Significance of large area of tympanic membrane – The area of tympanic is much larger than area of stapes footplate, which helps in converting sound of greater amplitude but lesser force to that of lesser amplitude and great force.
Lever ratio of tympanic membrane is:
| A |
1.4-1 |
|
| B |
1.3-1 |
|
| C |
18.2-1 |
|
| D |
1.5-1 |
Lever-Action of Ossicles
Handle of malleus is 1.3 times longer than process of the incus which constitutes for the lever-action.
Area Ratio:The area ratio of tympanic membrane is 14:1
Lever ratio = 1.3: 1
= Their product is 18:1 i.e. the pressure exerted at oval window.
This helps in the transformer action of the middle ear (impedance matching mechanism) i.e. converting sound of greater amplitude and less force to that of lesser amplitude but greater force.
| A |
Auriculotemporal |
|
| B |
Lesser occipital |
|
| C |
Greater occipital |
|
| D |
Parasympathetic ganglion |
After rupture of tympanic membrane, the hearing loss is:
| A |
10-40 dB |
|
| B |
5-15 dB |
|
| C |
20 dB |
|
| D |
300 dB |
Post head injury, the patient had conductive deafness and on examination, tympanic membrane was normal and mobile. Likely diagnosis is:
| A |
Distortion of ossicular chain |
|
| B |
Hemotympanum |
|
| C |
EAC sclerosis |
|
| D |
Otosclerosis |
- Fracture temporal bone (more commonly longitudinal) extending to external canal: tympanic membrane is frequently torn and inner ear is spared.
- Blood or CSF in external and middle ear.
- Damage to ossicle (most frequent being incudo-stapedial joint) resulting in more severe and permanent conductive deafness.
- Aseptic necrosis of long process of incus can lead to late conductive deafness.
Tympanic membrane is normal and mobile: In hemotympanum – tympanic membrane will appear red/blue (due to presence of blood pigments) so it is ruled out. … Logan Tumer1Oth/ed p441 Otosclerosis and EAC sclerosis do not occur in case of head injury and hence they are ruled out
| A | ASOM | |
| B |
Otosclerosis |
|
| C |
Tympanosclerosis |
|
| D |
Cholesteatoma |
Keratosis Obturans (Primary canal cholesteatoma)
- It is accumulation of a large plug of desquamated keratin in the external auditory meatus
- Seen between 5 and 20 yrs of age (i.e. younger age as compared to cholestealoma which is seen in middle age)
- May be U/L or Bilateral (occasionally)
- It may be associated with bronchiectasis and chronic sinusitis.
Clinical Features
- Pain in the ear (severe olatagia)
- Hearing loss (of conductive type)
- Tinnitus
- Ear discharge – sometimes
- Pearly white mass of keratin is visible in the ear canal
- Tympanic membrane is thickened and chalky white in appearance
- Ear canal is ballooned
Treatment
- Removal by syringing / Instrumentation
- Periodic checkup should be done to see reaccumulation
- If it recurs – keratolytic agent – 2% salicylic acid in alcohol can be tried.
| A | Handle of malleus appearance foreshortened | |
| B |
Cone of light is absent or interrupted |
|
| C |
Lateral process of malleus becomes more prominent |
|
| D |
None |
Ans. D None Ref. Dhingra sth/ed pg 61-62, 6th/eq P?5
Retracted Tympanic Bembrane
It is the result of-negative intratympanic pressure when Eustachian tube is blocked
Characteristics
It appears dull and lusterless
Cone of light is absent or interrupted
Handel of malleus appears foreshortened
Lateral process of malleus becomes more prominent
Anterior and posterior malleal folds become sickle shaped
It is immobile or has limited mobility when tested with pneumatic otoscope or siegle’s speculum.
Features of Normal Tympanic Membrane
It is shiny and pearly grey in colour
Has concavity on its lateral surface
Cone of light seen inantero – inferior quadrant
It’s transparency varies
It is mobile when tested with pneumatic otoscope or siegle’s speculum.
Dysfunction of tympanic membrane is characterized by all except:
| A |
Normal ‘cone of light’ |
|
| B |
Retracted TM |
|
| C |
Non prominent umbo |
|
| D |
Prominent malleolar folds |
Retracted Tympanic Membrane
It is the result of negative intratympanic pressure when Eustachian tube is blocked
Characteristics
It appears dull and lusterless
Cone of light is absent or interrupted
Handel of malleus appears foreshortened
Lateral process of malleus becomes more prominent
Anterior and posterior malleal folds become sickle shaped
It is immobile or has limited mobility when tested with pneumatic otoscope or siegle’s speculum.
Features of Normal Tympanic Membrane
- It is shiny and pearly grey in colour
- Has concavity on its lateral surface
- Cone of light seen in antero — inferior quadrant
- It’s transparency varies
- It is mobile when tested with pneumatic otoscope or siegle’s speculum.
Most common perforation site in tympanic membrane in ASOM:
| A | Antero-inferior | |
| B |
Postero-inferior |
|
| C |
Antero-superior |
|
| D |
Postero-superior |
Bluish tympanic membrane is seen in:
| A |
Early ASOM |
|
| B |
Glue ear |
|
| C |
Cholesteatoma |
|
| D |
Cholesterol granuloma |
In glue ear (serous otitis media) Tympanic membrane is dull opaque with loss of light reflex and appears yellow / grey / blue in colour.
- Normal colour of tympanic membrane is pearly grey.
- Congested membrane with prominent blood vessels (cartwheel sign) is seen in early stages of acute otitis media.
- Bluish discoloration is seen in haemotympanum.
- Flamingo pink color is seen in otosclerosis.
| A |
Attic |
|
| B |
Marginal |
|
| C |
Subtotal |
|
| D |
Total |
Treatment of choice for Perforation in pars flaccida of the tympanic membrane with cholesteatoma is:
| A |
Myringoplasty |
|
| B |
Modified Radical Mastoidectomy [MRM] |
|
| C |
Antibiotics |
|
| D |
Radical mastoidectomy |
Ans. B MRM
The aim of treatment is to produce a safe and dry ear and if possible to restore or improve the hearing. Myringoplasty should be done to close the perforation in the tympanic membrane. Which are central. But for pars flaccida perforation MRM is indicated.
A-7 year child presenting with acute otitis media, does not respond to ampicillin. Examination reveals full and bulging tympanic membrane, the treatment of choice is:
| A |
Sytemic steroid |
|
| B |
Ciprofloxacin |
|
| C |
Myringotomy |
|
| D |
Cortical mastoidectomy |
Indications of myringotomy in acute otitis media:
- Drum is bulging + acute pain.
- Incomplete resolution despite antibiotics when drum remains full with persistent conductive deafness.
- Persistent effusion beyond 12 weeks.
| A |
Myringotomy with penicillin |
|
| B |
Myringotomy with grommet |
|
| C |
Only antibiotics |
|
| D |
Wait and watch |
Fever + earache + congested and bulging tympanic membrane in a four year old child points towards Acute suppurative otitis media as the diagnosis.
Antibiotics (Penicillin) form the mainstay of treatment of acute otitis media and should be administered in a child with Acute otitis media and once tympanic membrane is bulging, myringotomy should be done.
Grommet insertion is not indicated in Acute suppurative otitis media. It may be used in cases of myringotomy for serous or secretory otitis media.
| A |
Middle ear |
|
| B |
Internal ear |
|
| C |
Eustachian tube |
|
| D |
Tympanic membrane |
Surgery on ear drum is done using:
| A |
Operative microscope |
|
| B |
Laser |
|
| C |
Direct vision |
|
| D |
Blindly |
Myringotomy is:
| A |
Surgical opening in Eustachian tube |
|
| B |
Surgical opening in tympanic membrane |
|
| C |
Surgical opening in semicircular canal |
|
| D |
None |
- Myringotomy is a surgical procedure of the eardrum or tympanic membrane.
- The procedure is performed by making a small incision with a myringotomy knife through the layers of tympanic membrane.
- This surgical procedure permits direct access to the middle ear space and allows the release of middle-ear fluid, which is the end product of otitis media with effusion (OME), whether acute or chronic.
What is tympanoplasty?
| A |
Eradication of middle ear disease with reconstruction of tympanic membrane & ossicles |
|
| B |
Eradication of disease from internal ear |
|
| C |
Eradication of middle ear disease with repair of tympanic membrane only |
|
| D |
Eradication of middle ear disease with repair of ossicles only |
Tympanoplasty (Tympanum = Middle ear)
It is an operation in which reconstructive procedure is limited to repair of tympanic membrane perforation.
Myringoplasty
It is an operation in which reconstructive procedure is limited to repair of tympanic membrane perforation.
Meatoplasty
Meatoplasty is an operation in which a crescent of conchal cartilage is excised to widen the meatus.
| A |
Hearing aid |
|
| B |
Stapedectomy |
|
| C |
Sodium fluoride |
|
| D |
Gentamicin |
Gentamicin is used to treat Meniere’s disease.
| A |
Tinnitus |
|
| B |
Vertigo |
|
| C |
Conductive deafness |
|
| D |
Fullness in ear |
A ruptured eardrum (tympanic membrane perforation) is a hole or tear in the thin tissue that separates your ear canal from your middle ear (eardrum).
A ruptured eardrum can result in hearing loss. It can also make your middle ear vulnerable to infections.
Blue ear drum is seen in:
| A |
Tympanosclerosis |
|
| B |
Secretory otitis media |
|
| C |
Otosclerosis |
|
| D |
Myringitis bullosa |
- The “blue ear drum” generally refers to a condition in which blood or blood products are found in the middle ear.
- After all possible causes for hemotympanum, including blood dyscrasias and trauma are searched for and ruled out, the patient may have chronic serous otitis media accompanied by bloody effusion.
- Treatment for all of these patients is conservative, consisting of medical therapy and, if need be, myringotomy and insertion of ventilation tubes.
- In spite of proper treatment, rarely the condition may progress, over a long period of time, to a state of intractability. Characteristic findings are a hypocellular mastoid, hyperplastic and metaplastic mucoperiosteal lining, including the presence of glands and cysts and Cholesterin granuloma.
- The recommended procedure is a modified radical mastoidectomy, placement of silicone rubber sheeting in the middle ear and insertion of a ventilation tube.
- It is to be emphasized that mastoid surgery is rarely indicated for these patients and only after all else has failed.
A 31 year old female patient complains of bilateral impairment of hearing for the past 5 years. On examination, tympanic membrane is normal and audiogram shows a bilateral conductive deafness. Acoustic reflexes are absent. All constitute part of treatment EXCEPT:
| A |
Hearing aid |
|
| B |
Stapectomy |
|
| C |
Sodium fluoride |
|
| D |
Gentamycin |
There is no medical treatment that cures otosclerosis.
Sodium fluoride has been tried to hasten the maturity of active focus and arrest further cochlear loss, but controversies exist and this treatment is NOT recommended generally
Unilateral conductive hearing loss in a patient with history of head injury. On examination, tympanic membrane is normal and mobile. The cause for deafness could be
| A |
Collection of fluid in the middle ear |
|
| B |
Otosclerosis |
|
| C |
Dislocation of the incudostapedial joint |
|
| D |
ASOM |
Acquired causes of conductive hearing loss include:
- Perforation of tympanic membrane
- Fluid in the middle ear-acute otitis media, serous otitis media, hemotympanum
- Mass in the middle ear (benign/malignant)
- Disruption of ossicles-trauma to ossicular chain, CSOM, cholesteatoma
- Fixation of ossicles-otosclerosis, tympanosclerosis
- Eustachian tube blockage
| A | Tubercular Otitis Media | |
| B |
Syphilitic Otitis Media |
|
| C |
Pseudomonas infection |
|
| D |
Fungal Otitis Media |
Ans. is ‘a’ i.e., Tubercular otitis media
Tubercular otitis media
- Tuberculosis of middle ear is a comparatively rare entity usually seen in association with or secondary to pulmonarytuberculosis, infection reaches the middle ear through eustachian tube.
- The rare modes of infection are through hematogenous spread from tubercular focus in lung, tonsils, cervical lymph nodes; or due to ingestion of infected cow’s milk.
- It usually affects children and young adults.
Clinical features
- Generally, tuberculosis of middle ear is unilateral.
- It is characterized by painless otorrhoea which fails to respond to the usual antimicrobial treatment. There is painless watery otorrhea.
- Single or multiple perforation of tympanic membrane. There may be multiple perforations in the early stages, but they coalesce into a large tympanic membrane perforation accompanied by a pale granulation tissue.
- Periauricular fistulae, lymphadenopathy and facial palsy are infrequent findings.
- Late complications include facial paralysis, labyrinthitis, postauricular fistulae, subperiosteal abscess, petrous apicitis and intracranial extension of infection.
| A | Presbycausis | |
| B |
Meniere’s disease |
|
| C |
Glue ear |
|
| D |
Acoustic neuroma |
Ans. is ‘c’ i.e., Glue ear
Among the given options, only glue ear (serous otitis media) is a cause of conductive deafness.
Patient with thin painless otorrhoea, multiple perforations of the tympanic membrane and failure to respond to antimicrobial treatment. What is the most probable causative organism ‑
| A |
Mycobacterium tuberculosis |
|
| B |
Staphylococcus aureus |
|
| C |
Candida albicans |
|
| D |
Aspegillusfumigatus |
Ans. is ‘a’ i.e., Mycobacterium tuberculosis
Thin painless otorrhoea, multiple perforations of the tympanic membrane and failure to respond to antimicrobial treatment are the features of tubercular otitis media and it is caused by Mycobacterium tuberculosis.
Tympanoplasty deals with reconstruction of –
| A |
Tympanic membrane |
|
| B |
Ossicular chain |
|
| C |
Both a and b |
|
| D |
None of the above |
Ans. is ‘c’ i.e., Both a and b
- Tympanoplasty is the surgical operation performed for reconstruction of tympanic membrane and/or middle ear ossicles.
- Myringoplasty is the reconstruction of tympanic membrane.
- Ossiculoplasty is the reconstruction of ossicular chain.
- Tympanoplasty = Myringoplasty ± ossiculoplasty
| A |
Tuberculous otitis media |
|
| B |
Fungal otitis media |
|
| C |
Serous otitis media |
|
| D |
Viral otitis media |
Ans. is ‘a’ i.e., Tubercular otitis media
Areas of spontaneously healed tympanic membrane are called ‑
| A |
Dimeric |
|
| B |
Pontiac |
|
| C |
Both of the above |
|
| D |
None of the above |
When a tympanic membrane heals spontaneously without grafting, perforation is closed by squamous epithelium before fibrous elements develop.
The fibrous layer may be attenuated or even lacking.
The resultant tympanic membrane has an area that lacks the tensile strength, elasticity, blood supply and resistance to future perforation of a fully reconstructed tympanic membrane.
Such areas are called dimeric because the squamous epithelium lies against the mucous membrane without intermediate fibrous elements.