CONGENITAL DISLOCATION OF THE HIP (CDH)
DEVELOPMENTAL DYSPLASIA OF HIP/ CONGENITAL DISLOCATION OF HIP
- Spontaneous dislocation of the hip.
- Occurring before, during or shortly after birth.
- Uncommon in India.
AETIOLOGY
- Hereditary predisposition to joint laxity
- Hormone induced joint laxity
- Breech malposition
PATHOLOGY
- 2 distinct types of dysplastic hips:
- dislocated at birth (classic CDH)
- dislocatable after birth
- Following changes are seen in a dislocated joint:
1. Femoral head is dislocated upwards and laterally;
- its epiphysis is small and ossifies late.
2. Femoral neck is excessively anteverted.
3. Acetabulum is shallow, with a steep sloping roof.
4. Ligamentum teres is hypertrophied.
5. Fibro- cartilaginous labrum of the acetabulum
- (limbus) may be folded into the cavity of the
- acetabulum (inverted limbus).
6. Capsule of the hip joint is stretched.
7. Muscles around the hip, especially the adductors, undergo adaptive shortening.
DIAGNOSIS
- Diagnosis is easy in an older child.
- Very difficult in younger children, especially during infancy.
CLINICAL FEATURES
- CDH is more common in first born babies, more on the left
- Common in females (M:F=1:5)
- Bilateral in 20% cases
- CDH may be detected at birth or soon after
- sometimes not noticed until the child starts walking.
- Following are the salient clinical features at different ages:
1. At birth: Routine screening of all newborns is necessary
- The examining paediatrician may notice signs suggestive of a dislocated or a dis- locatable hip.
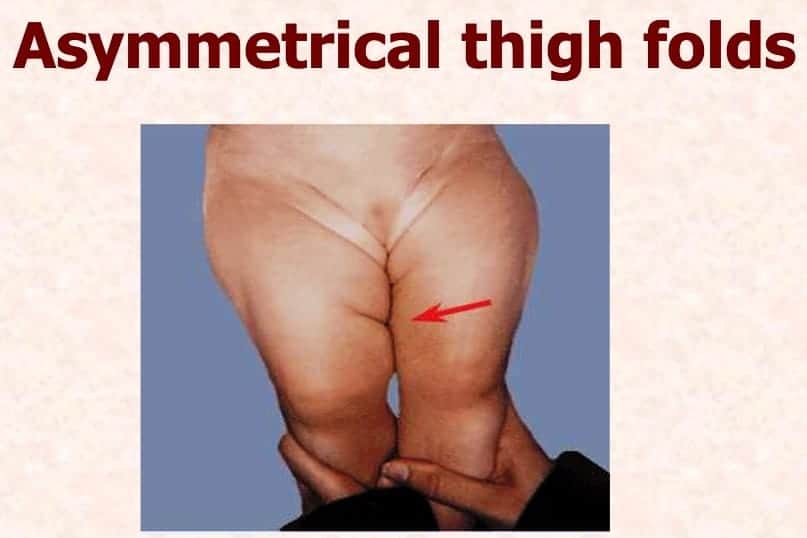
2. Early childhood: child is brought because the parents have noticed an asymmetry of creases of the groin.
- Limitation of movements of the affected hip, or a click everytime the hip is moved.
3. Older child:
- CDH may become apparent once the child starts walking.
- Parents notice that the child walks with a ‘peculiar gait’ though there is no pain.
- On examination a CDH may be found to be the underlying cause.
EXAMINATION
- Barlow’s test
- Ortolani’s test

In an older child, the following findings may be present:
Limitation of abduction of the hip.
Asymmetrical thigh folds
Higher buttock fold on the affected side.
Galeazzi’s sign:
- The level of the knees are compared in a child lying with hip flexed to 70° and knees flexed.
- There is a lowering of the knee on the affected side.

Ortolani’s test may be positive.
Trendelenburg’s test is positive
The limb is short and slightly externally rotated.

- There is lordosis of the lumbar spine.
Telescopy positive: In a case of a dislocated hip, it will be possible to produce an up and down piston-like movement at the hip.
- This can be appreciated by feeling the movement of the greater trochanter under the fingers.

A child with unilateral dislocation exhibits a typical gait in which the body lurches to the affected side as the child bears weight on it (Trendelenburg’s gait).
- In a child with bilateral dislocation, there is alternate lurching on both sides (waddling gait).
Some hip pathologies mimicking CDH are:
- Coxa vara, posterior hip dislocation and
- paralytic hip dislocation and
- paralytic hip dislocation
- Delayed appearance of the ossification centre of the head of the femur.
- Retarded development of the ossification centre of the head of the femur.
- Sloping acetabulum.
- Lateral and upward displacement of the ossification centre of the femoral head.
- A break in Shenton’s line

Exam Important
- Waddling gait due to Bilateral congenital dysplasia of hip.
- In an older child, the following findings may be present:
- Limitation of abduction of the hip.
- Asymmetrical thigh folds
- Higher buttock fold on the affected side.
- Galeazzi’s sign
- Ortolani’s test positive.
- Trendelenburg’s test is positive
- Telescopy positive
- Break in Shenton’s line

EXAMINATION OF CDH:
- Barlow’s test
- Ortolani’s test

Click Here to Start Quiz
