
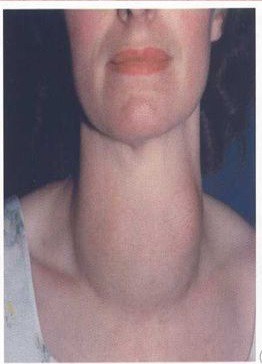
GOITER
GOITRE
DIFFUSE HYPERPLASTIC GOITER/ SIMPLE NON TOXIC/ COLLOID GOITER
- Usually seen at times of increased physiological demands as puberty, pregnancy.
- TSH stimulation ↑ (hyperthyroidism) → DHG → Colloid goitre
- Thyroid swelling moves on deglutition
- More common in females (15- 25yrs)

- Epidemiologically, goitre occurs in 2 forms-
a) Endemic-
- Prevalence of goitre in geographic area in more than 10% population.
- Endemic goiter caused mainly by lack of iodine.
- Endemic Goiter is ultimately caused by reduced thyroid hormone levels it is accompanied by the clinical syndrome of hypothyroidism.
b) Sporadic
MULTINODULAR GOITER (MNG)
- It is the end stage of hyperplastic goiter and is irreversible.
- Excessive metabolic demands cause an excessive enlargement of the thyroid gland.
- More common in females (4-5th decade)
CLINICAL FEATURES-
- Swelling infront of the neck
- Dyspnea and dysphagia
- Firm nodular thyroid
- Most common site of a nodule is at the junction of isthmus with one lobe
- Superior vena cava obstruction
- Recurrent laryngeal nerve palsy cases hoarseness.
- Pemberton’s sign à Increase pressure in thoracic inlet.

COMPLICATIONS-
- Painful nodule due to haemorrhage
- 4-10% MNG may convert into Follicular carcinoma
- Toxic MNG is also called Plummer’s disease.
INVESTIGATIONS-
- Complete blood picture
- X-ray shows calcification present.
- Flexible laryngoscopy shows vocal cord mobility
- Ultrasonography- standard investigations. Useful in solitary nodule, detects lymph nodes in the neck.
- FNAC- detects for malignancy
- T3, T4 and TSH levels.
- For nodules with more suspicious imaging characteristics (e.g., hypoechogenicity, microcalcifications, irregular margins),
biopsy is recommended when ≥1 cm.

TREATMENT-
- Subtotal thyroidectomy
- Total thyroidectomy (choice of today)- Patient who has had previous irradiation of the thyroid gland
- Lobectomy (Dunhill procedure)
- Small goiter- tab thyroxine (Eltroxin)- 0.1 to 0.2 mg/day
- Large goiter- 131I used in elderly to reduce size in elderly.
- Contrast agents and Iodine containing substance should be avoided as it induces Jod- Basedow Effect characterised by increased thyroid hormone production by autoimmune nodules.
Exam Important
- Epidemiologically, goitre occurs in 2 forms-
a) Endemic-
- Prevalence of goitre in geographic area in more than 10% population.
- Endemic goiter caused mainly by lack of iodine.
- Endemic Goiter is ultimately caused by reduced thyroid hormone levels it is accompanied by the clinical syndrome of hypothyroidism.
b) Sporadic
MNG
CLINICAL FEATURES-
- Swelling infront of the neck
- Dyspnea and dysphagia
- Firm nodular thyroid
- Most common site of a nodule is at the junction of isthmus with one lobe
- Superior vena cava obstruction
- Recurrent laryngeal nerve palsy cases hoarseness.
- Pemberton’s sign à Increase pressure in thoracic inlet.
COMPLICATIONS-
- Painful nodule due to haemorrhage
- 4-10% MNG may convert into Follicular carcinoma
- Toxic MNG is also called Plummer’s disease.
INVESTIGATIONS-
- Complete blood picture
- X-ray shows calcification present.
- Flexible laryngoscopy shows vocal cord mobility
- Ultrasonography- standard investigations. Useful in solitary nodule, detects lymph nodes in the neck.
- FNAC- detects for malignancy
- T3, T4 and TSH levels.
- For nodules with more suspicious imaging characteristics (e.g., hypoechogenicity, microcalcifications, irregular margins),
biopsy is recommended when ≥1 cm.
TREATMENT-
- Subtotal thyroidectomy
- Total thyroidectomy (choice of today)- Patient who has had previous irradiation of the thyroid gland
- Lobectomy (Dunhill procedure)
- Small goiter- tab thyroxine (Eltroxin)- 0.1 to 0.2 mg/day
- Large goiter- 131I used in elderly to reduce size in elderly.
- Contrast agents and Iodine containing substance should be avoided as it induces Jod- Basedow Effect characterised by increased thyroid hormone production by autoimmune nodules.
Don’t Forget to Solve all the previous Year Question asked on GOITER
