
HEPATORENAL SYNDROME
HEPATORENAL SYNDROME
- HRS is development of acute renal failure due to severe hepatic (advanced cirrhosis) or bilary disease with jaundice.
- Low cardiac putput and high plasma rennin predicts development of HRS.
- Patient develops oliguria, azotaemia and hyponatraemia.

ETIOLOGY-
- Bile salt sludging in the tubules
- Absorption of toxins
- Increase ADH release
- Hypoperfusion and renal ischaemia
- Precipitated by surgery, stress
PATHOLOGY-
- Increase in renal vascular resistance along with reduction in systemic vascular resistance
- Pathogenic marker is intense renal vasoconstriction with vasodilatation
INVESTIGATIONS-

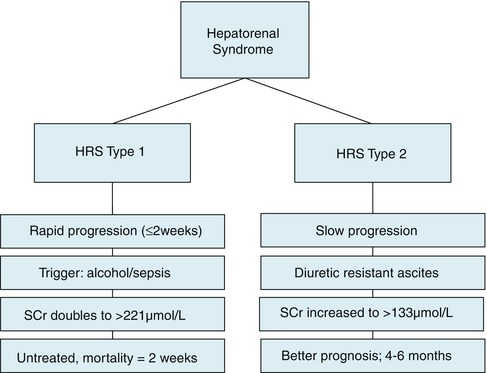
TYPES-
1. Type 1 HRS-
- Oliguria
- Decrease serum creatinine
- Poor prognosis
- No proteinuria
- Urine sodium excretion <10mmol/day
- Urine/ plasma osmolarity ration >1.5
Treatment-
- Albumin + terlipressin
2. Type 2 HRS
- Refractory ascites
- Better prognosis
- Increase serum creatinine levels
Treatment-
- Terlipressin- DOC
- Midodrine + pctreotide + IV albumin- reverse renal failure
- Best therapy for HRS- liver transplantation
- Dopamine or prostaglandin analogues for renal vasodilation
Exam Important
PATHOLOGY-
- Increase in renal vascular resistance along with reduction in systemic vascular resistance
- Pathogenic marker is intense renal vasoconstriction with vasodilatation
INVESTIGATIONS-
TYPES-
1. Type 1 HRS-
- Oliguria
- Decrease serum creatinine
- Poor prognosis
- No proteinuria
- Urine sodium excretion <10mmol/day
- Urine/ plasma osmolarity ration >1.5
Treatment-
- Albumin + terlipressin
2. Type 2 HRS
- Refractory ascites
- Better prognosis
- Increase serum creatinine levels
Treatment-
- Terlipressin- DOC
- Midodrine + pctreotide + IV albumin- reverse renal failure
- Best therapy for HRS- liver transplantation
- Dopamine or prostaglandin analogues for renal vasodilation
Don’t Forget to Solve all the previous Year Question asked on HEPATORENAL SYNDROME
