


LANGERHANS CELL HISTIOCYTOSIS (LCH)
LANGERHANS CELL HISTIOCYTOSIS.
- Previously referred to as “Histiocytosis X”.
- Before identifying “unknown X”; X refers to Langerhans,
- Langerhans cells are dendritic cells functioning as antigen presenting cells, present mostly in skin – epidermis.
- Unusual proliferation of immature dendritic cells called “Langerhans cell histiocytosis”.
- Considered neoplastic with oncogenetic mutations of BRAF.
Pathological morphology:
- Proliferating Langerhans cells contain,
- Abundant, vacuolated cytoplasm.
Birbeck granules –
- Present in cytoplasm.
- Are pentalaminar tubules with dilated terminal end producing “tennis racket-like appearance” (electron microscope).


- Vesicular “reniform shaped” nuclei with linear folds/grooves resulting in “Coffee-bean appearance”.
- Nuclei of Langerhans giant’s cells are arranged around periphery.


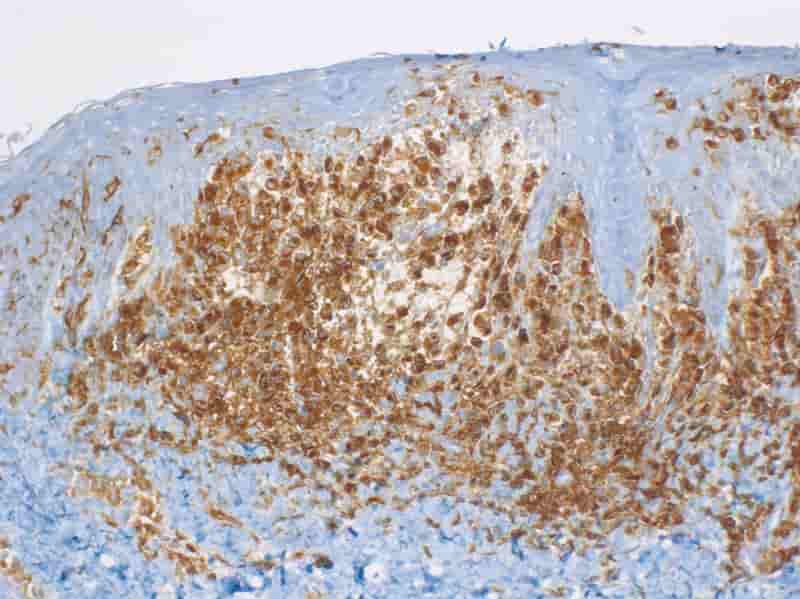
Tumor markers:
- Tumor cells express HLA-DR, S-100, CD1a. (Image below)
- Normal epidermal Langerhans cells express CCR6.
- Neoplastic cells express CCR6 & CCR7.

CLINICOPATHOLOGIC ENTITIES:
1. Letterer-Siwe disease
- Mostly < 2 years of age.
- Aggressive form with an increased risk of lymphoma.
- Bad prognosis.
Multifocal, multisystem LCH
- Characterized by multiple system involvement.
- Includes hepatosplenomegaly, lymphadenopathy pulmonary lesions & destructive bone lesions involving all bones simultaneously.
- Extensive bone marrow infiltration leads to pancytopenia.
- Most common presentation is cutaneous lesions resembling seborrheic dermatitis.
2. Eosinophilic granuloma:
- Peak incidence: 5-15 years.
Unifocal & uni-system LCH
- Involvement is restricted to single system
- Affects mostly skeletal system (particularly arise from medullary cavities of bone) which may be unifocal or multifocal.
- Most commonly affected bones are skull, vertebrae, ribs, clavicle, and femur.
- Eosinophils are usually prominent.
- Posterior pituitary stalk involvement causes Diabetes Insipidus.
3. Hand Schuller-Christian triad:
- Occurs in children below 5 yrs.
- Peak incidence: 2-10 years.
Clinical presentation:
- Calvarial bone defects
- Diabetes Insipidus
- Exophthalmos
4. Pulmonary LCH:
- Mostly in adult (20-40 years).
- Particularly affects smokers.
- Regress spontaneously after smoking cessation.
- Most prominent in upper & middle lung zones.
- X-ray: Bilateral, symmetric ill-defined nodules.
- Considered neoplastic due to BRAF mutations.
Treatment:
- Treatment is guided by extent of disease.
- Solitary bone lesion may be amenable through excision or limited radiation.
Radiation dosage:
- For children: 5-10 Gys.
- For adults: 24-30 Gys.
- Systemic diseases often require chemotherapy.
Exam Important
- Peak incidence is less than 3 years of age in Letterer Siwe disease type of Langerhans cell histiocytosis.
- Langerhans cell histiocytosis is radiosensitive.
- Diffuse form of Langerhans cell histiocytosis is known as Letterer Siwe disease.
- Langerhans cell histiocytosis produces a seborrheic dermatitis-like lesion in an infant.
- CD 1a is a marker of Langerhans cell histiocytosis.
- The nuclei of Langerhans giants’ cells are arranged around the periphery.
- Localised Langerhans cells histiocytosis affecting head & neck is called Eosinophilic Granuloma.
- X-bodies called Birbeck granules are characteristically seen in Langerhan’s cell granulomatosis.
- The histologic hallmark of Langerhans cells is Birbeck granules.
- Langerhans histiocytosis can be associated with diabetes insipidus.
- Hand Schuller Christian disease, Eosinophilic granuloma, Letterer Siwe disease are the types of Langerhan’s cell histiocytosis.
- Langerhans cells belong to Antigen presenting cells.
Don’t Forget to Solve all the previous Year Question asked on LANGERHANS CELL HISTIOCYTOSIS (LCH)

