
Leprosy Classification-Madrid and Ridley and Jopling Classification
CLASSIFICATION OF LEPROSY
Madrid classification
- Lepromatous(extreme form)
- Tuberculiod(extreme form)
- Dimorphous
- Interminate
- Pure neuritic(additional type in Indian classification
Ridley and Jopling Classification(Clinical, bacteriological, immunological, histological classification)
- Tuberculiod
- Boderline Tuberculiod
- Boderline borderline
- Boderline Lepromatous
- Lepromatous
|
SYMPTOMS
|
HISTOLOGICAL FEATURES
|
- Can be either one large red patch with well-defined raised borders or a large hypopigmented asymmetrical spot
- Non caseating granuloma in nerve
- Lesions become dry and hairless
- Loss of sensation may occur at site of some lesions
- Tender, thickened nerves with subsequent loss of function are common
- Spontaneous resolution may occur in a few years or it may progress to borderline or rarely
- neural involvement occurs early and may be pronounced
|
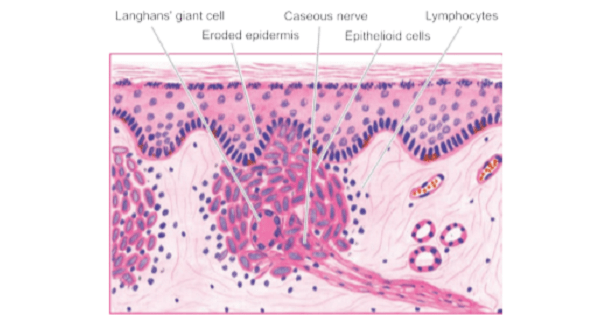
- Epithelioid cells
- lymphocytes
- giant cells form noncaseating granulomas.
- Dermal nerves are destroyed. Normal skin organs (e.g., sweat glands, hair follicles) are lost.
- ENL reaction seen
- Bacilli are frequently absent
- Max. no. of CD4 – T cells (TH -1)
|
| |
- Similar to tuberculoid type except that lesions are smaller and more numerous
- Normoesthetic and symmetrical lesions
- Disease may stay in this stage or convert back to tuberculoid form, or progress
|
- BT leprosy, granulomas are epithelioid, with a preponderance of lymphocytes. Dermal nerves are mostly destroyed. Bacilli may be scanty or absent.
|
- Numerous, red, irregularly shaped plaques
- Sensory loss is moderate
- Disease may stay in this stage, improve or worsen
- Asymmetrical thickening of
- several nerves.
- Several hypoesthetic macules on skin
- Lesions looking like inverted saucers are common
|
- granulomas are epithelioid
- dermal nerves may be visible
- bacilli are seen more often than in BT leprosy
|
- Numerous lesions of all kinds, plaques, macules, papules and nodules.
- Hypoesthetic
- Symmetrical nerve thickening; glove and stocking anesthesia
|
- histiocytes form granulomas
- dermal nerves are visible,
- bacilli are seen in greater number.
|
- Early nerve involvement may go unnoticed
- Normoesthetic, small, symmetrical and numerous lesions of all kinds, plaques, macules, papules and nodules
- Early symptoms include nasal stuffiness, discharge and bleeding, and swelling of the legs and ankles
|
- epidermis is normal
- rete flattened.
- clear space separates the epidermis from diffuse granulomatous reaction with macrophage
- large, foamy histiocytes (Virchow or lepra cells); and many intracellular AFB, which are frequently found in globi
- Epithelioid cells and giant cells are not found.
- Granulomas are most numerous around blood vessels, nerves, and skin appendages.
- Plasma cells are found
- Dermal nerves are easily visible.
- Max. no. of CD8 – T cells
|
If LL Left untreated, the following problems may occur:
- Leonine facies
- Ear lobes thicken, upper incisor teeth fall out
- Photophobia (light sensitivity), glaucoma and blindness
- Ucers
- Gynaecomastia:Testicles shrivel causing sterility and enlarged breasts (males)
- Internal organ infection causing enlarged liver and lymph nodes
- Saddle nose
- Voice becomes hoarse
- Slow scarring of peripheral nerves resulting in nerve thickening and sensory loss.
- Fingers and toes become deformed due to painless repeated trauma.
NERVES INVOLVED
- Propioception is carried by Goll & Burdech tract (posterior column)
- Which is not involved in leprosy
- Temperature & pain lost earlier than touch & pressure.
- Leprosy mainly affects peripheral nerves, eventually lit muscle wasting.
- Myopathy, muscle wasting may Vt abnormal EMGQ.
- Commanly involved nerves are:
- Posterior tibial (most common)
- Ulnar (2″ most common, most commonly Vt abscess)
- Peroneal/lateral popliteal
- Median & Facial
- Posterior auricular
- Supra orbital, supraclavicular,
Exam Question
Ridley and Jopling Classification(Clinical, bacteriological, immunological, histological classification
|
SYMPTOMS
|
HISTOLOGICAL FEATURES
|
- Can be either one large red patch with well-defined raised borders or a large hypopigmented asymmetrical spot
- Non caseating granuloma in nerve
- Lesions become dry and hairless
- Loss of sensation may occur at site of some lesions
- Tender, thickened nerves with subsequent loss of function are common
- Spontaneous resolution may occur in a few years or it may progress to borderline or rarely
- neural involvement occurs early
|
- Epithelioid cells
- lymphocytes
- giant cells form noncaseating granulomas.
- Dermal nerves are destroyed. Normal skin organs (e.g., sweat glands, hair follicles) are lost.
- ENL reaction seen
- Bacilli are frequently absent
- Max. no. of CD4 – T cells (TH -1)
|
| |
- Similar to tuberculoid type except that lesions are smaller and more numerous
- -Normoesthetic and symmetrical lesions
- -Disease may stay in this stage or convert back to tuberculoid form, or progress
|
- BT leprosy, granulomas are epithelioid, with a preponderance of lymphocytes. Dermal nerves are mostly destroyed. Bacilli may be scanty or absent.
|
- Numerous, red, irregularly shaped plaques
- Sensory loss is moderate
- Disease may stay in this stage, improve or worsen
- Asymmetrical thickening of
- several nerves.
- Several hypoesthetic macules on skin
- Lesions looking like inverted saucers are common
|
- granulomas are epithelioid
- dermal nerves may be visible
- bacilli are seen more often than in BT leprosy
|
- Numerous lesions of all kinds, plaques, macules, papules and nodules.
- Hypoesthetic
- Symmetrical nerve thickening; glove and stocking anesthesia
|
- histiocytes form granulomas
- dermal nerves are visible,
- bacilli are seen in greater number.
|
- Early nerve involvement may go unnoticed
- Normoesthetic, small, symmetrical and numerous lesions of all kinds, plaques, macules, papules and nodules
- Early symptoms include nasal stuffiness, discharge and bleeding, and swelling of the legs and ankles
|
- epidermis is normal
- rete flattened.
- clear space separates the epidermis from diffuse granulomatous reaction with macrophage
- large, foamy histiocytes (Virchow or lepra cells); and many intracellular AFB, which are frequently found in globi
- Epithelioid cells and giant cells are not found.
- Granulomas are most numerous around blood vessels, nerves, and skin appendages.
- Plasma cells are found
- Dermal nerves are easily visible.
- Max. no. of CD8 – T cells
|
If LL Left untreated, the following problems may occur:
- Leonine facies, Saddle nose
- Ear lobes thicken, upper incisor teeth fall out
- Photophobia (light sensitivity), glaucoma and blindness
- Testicles shrivel causing sterility and enlarged breasts (males)
- Internal organ infection causing enlarged liver and lymph nodes
- Renal lesion occurs,membranous glomerlonephritis .
- Voice becomes hoarse
- Slow scarring of peripheral nerves resulting in nerve thickening and sensory loss.
- Fingers and toes become deformed due to painless repeated trauma.
NERVES INVOLVED
- Propioception is carried by Goll & Burdech tract (posterior column)
- Which is not involved in leprosy
- Temperature & pain lost earlier than touch & pressure.
- Commanly involved nerves are:
- Posterior tibial (most common)
- Ulnar (2″ most common, most commonly Vt abscess)
Don’t Forget to Solve all the previous Year Question asked on Leprosy Classification-Madrid and Ridley and Jopling Classification
