Measurement Of Blood Pressure
MEASUREMENT OF BLOOD PRESSURE
- Blood pressure can be measured either directly & indirectly.
1. DIRECT METHOD/DIRECT MANOMETRY/INTRAARTERIAL METHOD:
- A catheterized artery connected to a mercury manometer/ pressure transducer/any other pressure-sensitive device.
- Accurate method.
- Yet, suitable only for experimental purposes.
- For clinical BP measurement, an indirect method preferred.
2. INDIRECT METHOD (USING SPHYGMOMANOMETER):
- Fairly accurate measurement.
- Non-invasive method.
METHOD:
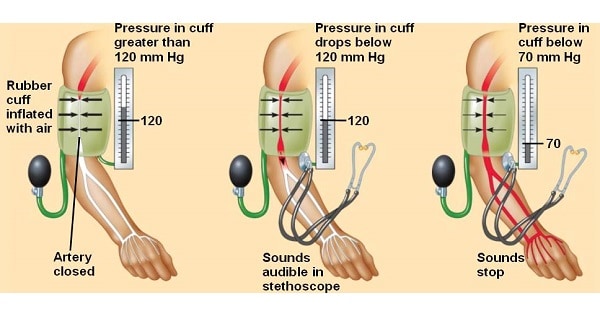
- An inflatable rubber/Riva-Rocci cuff attached to a mercury manometer.
- Wrapped around arm about an inch above cubital fossa.
- Cuff is rapidly inflated.
- Until pressure is well above expected systolic BP, so that brachial artery is occluded.
- Cuff pressure is lowered slowly at rate of 2-3 mm/sec.
- When it goes below systolic pressure, blood spurts through artery with each heartbeat.
- This marks systolic BP.
- On further lowering, blood flows through brachial artery relatively smoothly.
- Yet, still passes in spurts (since BP is at its lowest).
- Finally, when cuff pressure falls to level of diastolic pressure,
- Blood flow in brachial artery becomes entirely free from turbulence.
- This marks diastolic BP.
- Blood pressure measured by an auscultatory method using sphygmomanometer tends to be higher than true intra-arterial pressure measured by arterial cannulation.
- Because of some cuff pressure dissipating between cuff & artery in soft tissue.
IDEAL METHODOLOGY:
- While measuring BP, patient should be in resting position (seating or lying down).
- Patient’s arm with attached cuff shows be at heart level.
- Cuff should be applied to upper arm.
- Cuff should encircle at least 80% of arm.
- I.e. length of bladder should be at least 80% arm circumference.
- Cuff width should be at least 40% of circumference.
TYPES OF METHODOLOGY:
- Three different methods of performing sphygmomanometry –
- Oscillatory.
- Palpatory.
- Auscultatory.
- Difference is in criteria for identifying systolic & diastolic pressure.
1. OSCILLATORY METHOD:
- Here, mercury column is observed.
- As mercury column falls to touch systolic pressure, it starts showing small oscillations.
- Oscillations are largest at mean BP & abruptly disappear at diastolic pressure.
- Rarely used methodology.
2. PALPATORY METHOD:
- Here, radial artery pulse is palpated.
- As cuff pressure falls, pulse appears at systolic point.
- An inaccurate method.
- Results are about 2-5 mm Hg lower than those obtained through auscultatory method.
- Diastolic point cannot be identified by this method.
3. AUSCULTATORY METHOD:
- Method uses stethoscope, placed over brachial artery in cubital fossa.
- “Korotkoff’s sounds” appear at systolic pressure & disappear at diastolic pressure.
- Sounds are attributed to turbulence.
- Caused by partial arterial occlusion.
- According to Americal Heart Association, Korotkoff’s sound occurs in five phases:
- Onset of phase I Korotkoff’s sound corresponds to systolic pressure.
- Disappearance of sounds (phase V) corresponds to diastolic pressure.
Phase 1:
- Faint, clear, tapping sounds.
- This is systolic pressure.
Phase 2:
- Murmurs or swishing sounds.
Phase 3:
- Crisper, more intense sounds.
Phase 4:
- Distinct, abrupt muffle of sound.
- In children, this is Diastolic Pressure.
Phase 5:
- No sounds.
- This is diastolic pressure in adult.
AUSCULTATORY GAP:
- Phase I sounds sometimes disappears.
- Occurs when pressure is lowered from systolic pressure.
- Sounds reappear at a lower level.
- This, interval between systolic & diastolic when no Karotkof sound heard referred as “Auscultatory gap”.
- Mainly in hypertensive patients.
- If cuff pressure is not adequately elevated in beginning, lower limit of auscultatory gap can be mistaken as systolic BP.
- Hence, falsely low recording of systolic BP may occur.
- This error avoided by recording systolic BP through palpatory method.
CONDITIONS INCREASING BP:
1. Size of inflatable cuff:
- Is of critical importance.
- Selection of proper cuff size:
- Determined by limb dimensions for BP measurement.
Width of cuff:
- Should be 40% of circumference.
- Otherwise, 1.2 times diameter of extreme.
Length of inflatable cuff:
- Should be 80% of arm circumference.
- Ie., Length-to-width ratio of 2: 1.
False high BP (Pseudohypertension):
- Seen with using too narrow cuff/small cuff size
- Also in obese patients.
- Seen with thick calcified arteries.
- E.g., in elderly, atherosclerosis, diabetes & Monkenberg’s sclerosis.
- Vessels are difficult to compress & higher cuff pressure is required to compress them.
Falsely low BP:
- Using too wide a cuff will result in falsely low values.
METRICS:
BP AT VARIOUS PORTIONS OF CVS:
- Right ventricle – 25/0 mm Hg (Systolic/diastolic).
- Left ventricle – 120/0 mm Hg.
- Right atrium – 2 mm Hg.
- Left atrium (Pulmonary Capillary Wedge Pressure) – 5 mm Hg (4-10 mm Hg).
- Aorta – 120/80 mm Hg.
- Pulmonary artery – 25/8 mm Hg.
Exam Question
MEASUREMENT OF BLOOD PRESSURE
INDIRECT METHOD (USING SPHYGMOMANOMETER):
- Cuff is rapidly inflated until pressure is well above expected systolic BP so that brachial artery is occluded.
- Blood pressure measured by an auscultatory method using sphygmomanometer tends to be higher than true intra-arterial pressure measured by arterial cannulation.
- Because some cuff pressure gets dissipated between the cuff and artery in soft tissue.
IDEAL METHODOLOGY:
- While measuring BP, patient should be in resting position (seating or lying down).
- Patient’s arm with attached cuff shows be at heart level.
- Cuff should be applied to upper arm.
- Cuff should encircle at least 80% of arm.
- I.e. Cuff length of bladder should be at least 80% arm circumference.
- Cuff width should be at least 40% of the circumference.
TYPES OF METHODOLOGY:
1. PALPATORY METHOD:
- Diastolic point cannot be identified by this method.
3. AUSCULTATORY METHOD:
- Method uses stethoscope, placed over brachial artery in cubital fossa.
- “Korotkoff’s sounds” appear at systolic pressure & disappear at diastolic pressure.
- Sounds are attributed to turbulence.
- Caused by partial arterial occlusion.
- According to Americal Heart Association, Korotkoff’s sound occurs in five phases:
- Onset of phase I Korotkoff’s sound corresponds to systolic pressure.
- Disappearance of sounds (phase V) corresponds to diastolic pressure.
AUSCULTATORY GAP:
- Falsely low recording of systolic BP may occur.
CONDITIONS INCREASING BP:
1. Size of inflatable cuff:
- Width of cuff should be 40% of circumference/1.2 times diameter of extreme.
- Length of inflatable cuff should be 80% of arm circumference.
- Ie., Length-to-width ratio of 2:1.
Pseudohypertension:
- With usage of too narrow a cuff.
- In obese patients.
- Seen with thick calcified arteries.
- E.g., in elderly, atherosclerosis, diabetes & Monkenberg’s sclerosis.
BP AT VARIOUS PORTIONS OF CVS:
- Right ventricle – 25/0 mm Hg (Systolic/diastolic).
- Left ventricle – 120/0 mm Hg.
- Left atrium (Pulmonary Capillary Wedge Pressure) – 5 mm Hg (4-10 mm Hg).
Don’t Forget to Solve all the previous Year Question asked on Measurement Of Blood Pressure