
Paracetamol
INTRODUCTION:
- Paracetamol has good analgesic & antipyretic properties.
- Has minimal anti-inflammatory action compared to other NSAIDs.
- Due to ineffective peroxidases synthesis at inflammatory sites.
- Kit B given at subcentre is Paracetamol.
MOA:
- Selective COX3 inhibitors.
- May also inhibit prostaglandin biosynthesis in CNS but not in peripheral tissues.
PHARMACOKINETICS:
|
||||||||||||
- Bioavailability is significantly lower when given rectally.
INDICATIONS:
Treatment of pains of all kinds including,
- Headaches, dental pain, postoperative pain, pain in connection with colds, post-traumatic muscle pain).
- Also for migraine headaches, dysmenorrhea & joint pain.
In cancer patients –
- Used for mild pain.
- Can be administered in combination with opioids (e.g. codeine).
DOSE:
|
||||||||||||||||||||||
TOXIC DOSES:
- More than 7.5 gm(around 15 tablets)- minimal toxicity
- If >15 gm (30 tablets)- severe toxicity
- In adult- toxic dose is 150 mg/kg
- In children, toxic dose is 200 mg/kg
- In presence of chronic disease or malnutrition, even 2gm of paracetamol can be toxic.
ADVANTAGES:
- Comparative to other analgesics have less GI toxicity.
- Preferred alternative to aspirin (acetylsalicylic acid – e.g. because of history of ulcer or viral infection in child).
- Considered equipotent to aspirin (acetylsalicylic acid)
- Also well suited for use in children.
ADVERSE EFFECTS:
- Blood dyscrasia (e.g. thrombocytopenia), methemoglobinemia, and hemolytic anemia – Very rare.
- Fixed drug eruption – Cutaneous reaction to an ingested drug with characteristic clinical features.
- Sterile pyuria
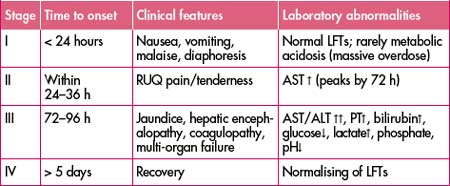
PARACETAMOL POISONING:
- When durg is metabolized in liver, small amounts of an intensely active metabolite, which is normally immediately inactivated by glutathione, are produced.
- An overdose causes a glutathione deficiency; the reactive metabolite may then cause hepatocellular damage and necrosis leading to acute liver failure.
- Toxic effects have been observed in adults treated with doses of more than 10 g (20 tablets).
- However, if there is a pre-existing liver insufficiency, paracetamol can be hepatotoxic even in small amounts.
- Paracetamol poisoning can cause metabolic acidosis
- Vomiting, pain in abdomen, jaundice, and encephalopathy.
- History of attempt to commit suicide.
PRECAUTIONS:
- The antidote acetylcysteine (e.g. fluimucil) must be administered within 8 to 10 hours when there is intoxication: i.v. infusion of 150 mg/kg in 15 minutes, then 50 mg/kg for 4 hours, and then 100 mg/kg for 16 hours in a 5% glucose solution.
PCM Poisoning:
TREATMENT:
Regimen for Acetylcysteine:
- 150mg/kg in 200 ml 5% dextrose over 15 min
- 50mg/kg in 500 ml 5% dextrose over next 4 hours
- 100mg/kg in 1 L 5% dextrose over ensuing 16 hours
- Total dose : 300mg/kg over 20.25 hrs
Exam Question
- Paracetamol poisoning produces Metabolic acidosis
- Vesiculobullous lesion healed with hyperpigmentation on the glans soon after taking tablet paracetamol for fever suggest Fixed drug eruption
- In cases of moderate to severe poisoning of paracetamol, N-acetyl cysteine (mucomyst) should be given orally within 24 hours of overdose to prevent hepatic damage.
- Paracetamol is one of the safest NSAIDs produces very little GI toxicity and can be administered in patients intolerant to other NSAIDs.
- Kit B given at subcentre is Paracetamol
- Sterile pyuria may occur due to Paracetamol
- A patient presented with vomiting, pain in abdomen, jaundice and encephalopathy. There is a history of attempt to commit suicide. Poisoning suspected is Paracetamol
Don’t Forget to Solve all the previous Year Question asked on Paracetamol