

Sideroblastic anaemia
SIDEROBLASTIC ANAEMIA
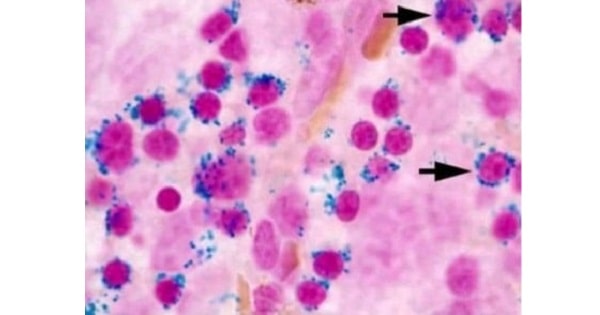
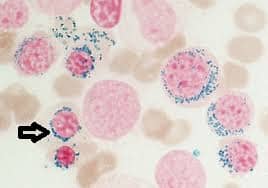
- Sideroblastic anaemia is a group of disorder in which erythroid precursor in the bone marrow show characteristic ‘ringed sideroblastic’.
- Siderocytes are erythrocytes & sideroblasts are normoblasts.
- Siderocytes contains granules of non- heme iron.
- Granules are positive with Prussian blue reaction & Romanowsky dyes called Pappenheimer bodies.
- Sideroblasts nucleated red cells.

TYPES OF SIDEROBLAST ANAEMIAS-
- Herediatry sideroblastic anaemia
- Rare X- linked disorder associated with defective enzyme aminolevulinic acid (ALA) synthetase for haem synthesis.
2. Acquired sideroblastic anaemia-
- Primary-
- Secondary-
- Alcohol & lead. (Sideroblastic anaemia is seen in chronic poisoning of lead)


Lab findings-
- Blood picture- hypochromic, microcytic.
- MCV, MCH, MCHC decrease in hereditary type.
- MCV increase in acquired type.
- Bone marrow examination- macronormoblastic erythropoiesis.
- Marrow iron stores increase.
- Pathognomonic ring sideroblasts present serum ferritin increase.
- Serum iron increase.
- Iron deposition increase.


TREATMENT-
- No definite treatment.
- Pyridoxine dose.
- Blood transfusion can be used for treatment.
Exam Important
- Sideroblastic anaemia is a group of disorder in which erythroid precursor in the bone marrow show characteristic ‘ringed sideroblastic’.
- Siderocytes are erythrocytes & sideroblasts are normoblasts.
- Siderocytes contains granules of non- heme iron.
- Granules are positive with Prussian blue reaction & Romanowsky dyes called Pappenheimer bodies.
TYPES OF SIDEROBLAST ANAEMIAS-
- Herediatry sideroblastic anaemia
- Rare X- linked disorder associated with defective enzyme aminolevulinic acid (ALA) synthetase for haem synthesis.
2. Acquired sideroblastic anaemia-
- Secondary- Drugs, chemical & toxins (Isoniazid- antituberculous drugs & pyridoxine antagonist).
- Alcohol & lead.
Lab findings-
- Blood picture- hypochromic, microcytic.
- MCV, MCH, MCHC decrease in hereditary type.
- MCV increase in acquired type.
- Bone marrow examination- macronormoblastic erythropoiesis.
- Marrow iron stores increase.
- Pathognomonic ring sideroblasts present serum ferritin increase.
- Serum iron increase.
- Iron deposition increase.

Don’t Forget to Solve all the previous Year Question asked on Sideroblastic anaemia

