MYCOTIC CORNEAL ULCER
| A | Big hypopyon | |
| B |
Sterile immune ring |
|
| C |
Corneal vascularisation |
|
| D |
Feathery finger like extensions into the stroma |
All of the following are signs of mycotic corneal ulcer, EXCEPT:
| A |
Big hypopyon |
|
| B |
Sterile immune ring |
|
| C |
Corneal vascularisation |
|
| D |
Feathery finger like extensions into the stroma |
- Dry looking, greyish white with elevated rolled out margins
- Feathery finger-like extensions into the surrounding stroma
- Presence of sterile immune ring
- Small satellite lesions around the ulcer
- Big hypopyon which may not be sterile
- Absent corneal vascularisation.
Branched septate hyphae found on corneal smear in a case of corneal ulcer is –
| A |
Candida |
|
| B |
Mucor |
|
| C |
Aspergillus |
|
| D |
Histoplasma |
Ans. is ‘c’ i.e., Aspergillus
- Septate hyphae and involvement of the cornea favours the diagnosis of the Aspergillus
- Aspergillus can cause Aspergillus keratitis after trauma to the cornea. The hyphae of Aspergillus are septate & branched.
- Mucor: It can cause infection of the eye but its hyphae are not septate.
- Candida: Candida can also involve the eye (it usually involves retina). Its infectious form is yeast, not hyphae.
- Histoplasma: Histoplasma has septate hyphae but it does not involve the eye.
Common fungus causing corneal ulcer ‑
| A | Aspergillus | |
| B |
Mucor |
|
| C |
Fusarium |
|
| D |
a and c |
Ans. is ‘a’ i.e., Aspergillus; ‘c’ i.e., Fusarium
Remember
Fungi which do not have Septate Hyphae belong to the family Zygomycetes. They are:
. Mucor . Pilobolus
. Rhizopus . Cunninghamella
. A bsidia
. Fungal infections of the cornea are secondary to injury, bacterial infection and treatment with antibacterial agents and steroids.
. Occur most often in hot climates.
. Caused by common saprophytic moulds- Aspergillus, Fusarium
| A | Satellite lesion | |
| B |
Symptoms more than signs |
|
| C |
Purulent ulcer |
|
| D |
All |
A. i.e. Satellite lesion
A 30 year old male presents with a history of injury to the eye with a leaf 5 days ago and pain, photophobia and redness of the eye for 2 days. What would be the most likely pathology?
| A |
Anterior uveitis. |
|
| B |
Conjunctivitis |
|
| C |
Fungal corneal ulcer. |
|
| D |
Corneal laceration. |
C i.e. Fungal Corneal ulcer
Features of fungal ulcer :
| A |
Symptoms more than signs |
|
| B |
Dry ulcer |
|
| C |
Diffuse corneal edema |
|
| D |
All |
B i.e. Dry ulcer
True about fungal corneal ulcer
| A |
Symptoms are severe |
|
| B |
Dry looking ulcer |
|
| C |
Satellite lesion |
|
| D |
b and c |
B i.e. Dry looking ulcer; C i.e. Satellite lesions
Which of the following will be the most important adjuvant therapy in a case of fungal corneal ulcer :
| A |
Atropine sulphate eye ointment |
|
| B |
Dexamethasone eye drops |
|
| C |
Pilocarpine eye drops |
|
| D |
Lignocaine eye drops |
A i.e. Atropine sulphate ointment
Which of the following is the drug of choice for treatment of corneal ulcers caused by filamentous fungi?
| A |
Itraconazole |
|
| B |
Natamycin |
|
| C |
Nystatin |
|
| D |
Fluconazole |
B i.e. Natamycin
Which of the following is not true regarding fungal corneal ulcer:
March 2009
| A |
Convex hypopyon |
|
| B |
Commonly perforates |
|
| C |
Hyphate margins |
|
| D |
Satellite lesions are seen |
Ans. B: Commonly perforates
- Causative fungi:
- Filamentry fungi – include- Aspergillus, fusarium, cephalosphorium, curvuluria, penicillium.
- Yeast – Candida, Cryptococcus
Mode of infection:
- Injury by vegetative materials (Common sufferers are field workers specially in harvesting season)
- Injury by animal tail
- Secondary fungal ulcer – is commonly found in immunosuppresed hosts.
Patients who are suffering from dry eye, herpetic Keratitis, bullous keratopathy and Post-operative case of keratoplasty Fungi do not infect the cornea easily – they require trauma, immunological compromised state & tissue devitalization. Fungal corneal infections tend to spread deep into the corneal stroma, where the organisms are inaccessible to the usual diagnosis and therapeutic measure.
Fungi even may penetrate an intact Descement’s membrane into the anterior chamber.
Clinical features:
- Pain
- Watering – reflex hyperlacrimation
- Photophobia – Stimulation of nerve ending
- Redness – Congestion of circum-corneal vessels,
- Dry eye, grayish white with elevated rolled out margins
- Feathery figure like extension surround the stroma under intact epithelium, Yellow line demarcation (sterile immune ring) known as Wessley’s ring due to deposition of immune complex and inflammatory cell around the ulcer.
- Multiple small satellite lesions may present around the ulcer
- Hypopion – Big, thick, immobile, not sterile may be present
- Perforation – rarely
- Corneal vascularisation are conspicuously absent.
Diagnosis:
– Wet KOH
– Direct smear immediately fixed with methyl alcohol.
– Giemsa stain – Show ghosting of fungal wall and yeast budding is may be noted.
– Gomori methanamine Silver technique – Delineate the hyphae as sharp black structure against a pale green background.
– Gram stain – fungus can be seen directly
– Periodic acid schiff (PAS)
– Calco fluor white
| A | Herpetic keratitis | |
| B |
Atopic dermatitis |
|
| C |
Fungal corneal ulcer |
|
| D |
Exposure keratitis |
Ans. is ‘C’ i.e., Fungal corneal ulcer
- Topical corticosteroids enhance fungal replication and corneal invasion and therefore, contraindicated in a fungal corneal ulcer.
- Option ‘A’ requires specific mention here:-
- Topical corticosteroids are contraindicated in herpetic keratitis. But not in all forms of herpetic keratitis:-
- Epithelial herpetic keratitis (Dendritic ulcer, geographic ulcer) Topical corticosteroids are contraindicated.
- Stromal keratitis (Disciform & Diffuse necrotic) Topical corticosteroids along with topical antiviral drugs are used as the first line of treatment.
Note:
- If herpetic keratitis has given as the option, then look at other options. If any of the other options is a clear cut contraindication for corticosteroid (e.g. fungal corneal ulcer in this question), consider that option as your answer. If no other option is a contraindication for topical corticosteroid, consider herpetic keratitis as the answer.
- If dendritic ulcer is an option, consider it as the answer.
| A |
Fungal filaments |
|
| B |
Fungal spores |
|
| C |
Purulent material |
|
| D |
Sterile material |
Ans. is ‘a’ i.e., Fungal filaments
Hypopyon in fungal ulcer is not sterile as in bacterial corneal ulcer because the fungi penetrate in the anterior chamber without perforation.
Hypopyon in fungal ulcer is fixed and does not show positional variation as in bacterial corneal ulcer as the fungal filaments adhere to the walls of anterior chamber.
Which of the following is not a feature of a fungal corneal ulcer?
| A | The most common cause is Aspergillus. | |
| B |
A Big hypopyon is present. |
|
| C |
Symptoms are more pronounced than signs |
|
| D |
Feathery finger-like extensions are present |
Salient features of a fungal corneal ulcer:
- It is caused by trauma with vegetative or organic matter.
- Signs are more pronounced than symptoms.
- The corneal ulcer appears dry.
- Delicate feathery finger-like extensions are present.
- A sterile, immune ring (yellow line of demarcation) may be present
- Multiple, small satellite lesions may be present around the ulcer.
- Usually, a big hypopyon is present.
- Pigmented ulcer (brownish) may be caused by some dematiaceous species of fungi.
- Perforation in mycotic ulcer is rare but can occur.
- The most common cause is Aspergillus.
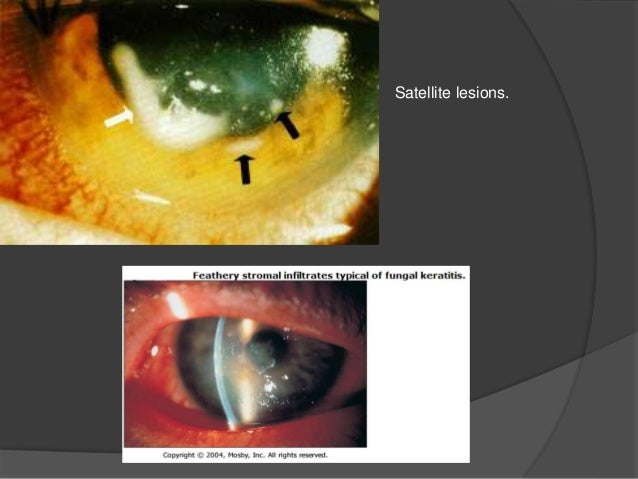
Image: Fungal corneal ulcer, indicating a satellite lesion
Immune ring is a feature of ?
| A |
Interstitial keratitis |
|
| B |
Fungal corneal ulcer |
|
| C |
Bacterial corneal ulcer |
|
| D |
Herpes simplex keratitis |
Ans. is ‘b’ i.e., Fungal corneal ulcer
Clinical features of fungal (mycotic) corneal ulcer
Symptoms are similar to bacterial corneal ulcers but in general, they are less marked than the equal-sized bacterial ulcer. On the other hand, signs are very prominent, i.e. signs are more prominent than symptoms. Following signs can be seen : –
- Greyish-white dry looking ulcer with the elevated rolled out feathery & hyphate margins.
- Feathery finger-like extension into surrounding stroma under the intact epithelium.
- A sterile immune ring (yellow line) of Wessely.
- Multiple small satellite lesions.
- Non-sterile (infected) hypopyon (Pseudohypopyon).
- Perforation is rare and corneal vascularization is conspicuously absent.
