

Endometrial Carcinoma
Fractional curettage is done in all except :
| A |
Endometrial carcinoma |
|
| B |
CA cervix |
|
| C |
Fibroid uterus |
|
| D |
As part of MTP |
Fractional curettage is done in all except :
| A |
Endometrial carcinoma |
|
| B |
CA cervix |
|
| C |
Fibroid uterus |
|
| D |
As part of MTP |
As part of MTP
Persistent anovulation not treated leads to all except :
| A |
Hirsutism |
|
| B |
Ovarian Carcinoma |
|
| C |
Endometrial Carcinoma |
|
| D |
Increased risk of CVS disease |
Persistent anovulation not treated leads to all except :
| A |
Hirsutism |
|
| B |
Ovarian Carcinoma |
|
| C |
Endometrial Carcinoma |
|
| D |
Increased risk of CVS disease |
- Ans. is b i.e. Ovarian carcinoma
Clinical Consequences of Persistent Anovulation
- Infertility°
- Menstrual bleeding problems ranging from amenorrhea to irregular, heavy bleeding° (DUB). Most common menstrual disorder associated with anovulation is oligomenorrhea.°
- Hirsutism°, Alopecia° and Acne.
- Increased risk of Endometrial cancer° and perhaps, Breast cancer°.
- Increased risk of Cardiovascular disease°.
- Increased risk of Diabetes mellitus° in patients with insulin resistance.
Extra Edge :
Recommended investigations in case of anovulatory hyperandrogenic women (to exclude specific causes and problems).
|
1. |
Thyroid stimulating hormone |
4. |
Screen for cushing disease |
|
2. |
Prolactin |
5. |
Endometrial biopsy |
|
3. |
Lipid and Lipoprotein profile |
6. |
Glucose tolerance |
|
|
|
7. |
Body mass Index. |
In the presence of clinical signs of excess androgen stimulation – Two tests which should be done are :
- Total testosterone levels
- 17 – hydroxy progesterone morning and fasting.
Poly cystic ovarian disease is associated with :
| A |
Ovarian cancer |
|
| B |
Endometrial carcinoma |
|
| C |
Congenital adrenal hyperplasia |
|
| D |
Vaginal carcinoma |
Poly cystic ovarian disease is associated with :
| A |
Ovarian cancer |
|
| B |
Endometrial carcinoma |
|
| C |
Congenital adrenal hyperplasia |
|
| D |
Vaginal carcinoma |
Endometrial carcinoma
All of the following are known risk factors for development of endometrial carcinoma except :
| A |
Obesity |
|
| B |
Family History |
|
| C |
Use of Hormone Replacement Therapy |
|
| D |
Early Menopause |
All of the following are known risk factors for development of endometrial carcinoma except :
| A |
Obesity |
|
| B |
Family History |
|
| C |
Use of Hormone Replacement Therapy |
|
| D |
Early Menopause |
Ans. is d i.e. Early menopause
Friends, this is the most frequently asked question on Endometrial cancer. Mug up predisposing factors by heart. Endometrial carcinoma occurs as a result of unopposed estrogen exposure in body.
Predisposing factors are :
Family Family history
Has Hypertension
m Obesity
L Late menopause / Early menarche Diabetes
A Atypical endometrial hyperplasia
U Unopposed estrogen or increased estrogen in body as in :
- HRT
- Fibroid
- PCOD
- Feminizing ovarian Tumour
N Nulliparity
H/o infertility / menstrual irregularity
Mnemonic : Family has OLD AUNT
- Oral contraceptive pills (combined addition of Progesterone to HRT).
- Smoking (as it decreases leygirtpf estrogen, decreases weight& is associated with earlier age at menopause).
- HRT
- Fibroid
- PCOD
- Feminizing ovarian Tumour
True about endometrial carcinoma :
| A |
Predisposed by diabetes mellitus, hypertension and obesity |
|
| B |
Adenosquamous type is commonest |
|
| C |
Commonly associated with Ca cervix |
|
| D |
Common age group affected is between 20-40 years |
True about endometrial carcinoma :
| A |
Predisposed by diabetes mellitus, hypertension and obesity |
|
| B |
Adenosquamous type is commonest |
|
| C |
Commonly associated with Ca cervix |
|
| D |
Common age group affected is between 20-40 years |
Ans. is a i.e. Predisposed by Diabetes mellitus, hypertension and obesity
Endometrial cancer :
- Most common in nulliparous females.°
- Age group : Peak incidence 60 years (6′”-7′h decade most common).°
But in 25% cases can occur before menopause or in young females.
- Race : Most common in Jews (Unlike Ca cervix).
- Predisposing Factors : Already discussed in detail earlier. A combination of hypertension, diabetes and obesity in association with Endometrial Ca is known as Corpus Cancer Syndrome.
- Associated diseases : — Fibroid uterus° (as it also occurs in Nulliparous females)
— Cervical Polyps°
Pathology : Most common variant is Adenocarcinoma° (known as Endometroid and not Adenosquamous). Only 15-20% of Adenocarcinomas may have squamous differentiation.
Histology :
Endometrial carcinoma can be distinguished from hyperplasia by :
- Back to back arrangement of Glands°
- No intervening stroma°
- Desmoplastic stroma
- Extensive papillary pattern Squamous epithelium differentiation° Clinical features : A female of perimenopausal age group( 6th -71” decade) presents with :
- Abnormal bleeding (90% cases) in the form of metrorrhagia menometrorrhagia, intermenstrual spotting, postmenopausal bledding
- Discharge (1%) P/V : — Brown, watery offensive discharge — Watery discharge free from blood (hydrorrhea°).
- Pelvic pressure/discomfort.
- Referred pain in hypogastrium or both iliac fossae (Simpson’s pain).Pain tsevere and tends to occur at the same time each day, lasting on 1-2 hrs (Important).
- In some older patients, bleeding may not occur due to cervical stenosis. causing hematometra/pyometra.
- Desmoplastic stroma°
- Extensive papillary pattern
- Squamous epithelium differentiation°
Clinical features : A female of perimenopausal age group( 6th -71” decade) presents with :
- Abnormal bleeding (90% cases) in the form of metrorrhagia menometrorrhagia, intermenstrual spotting, postmenopausal bledding.
- Discharge (1%) P/V : — Brown, watery offensive discharge
— Watery discharge free from blood (hydrorrhea°).
- Pelvic pressure/discomfort.
- Referred pain in hypogastrium or both iliac fossae (Simpson’s pain).
Pain tsevere and tends to occur at the same time each day, lasting on 1-2 hrs (Important).
In some older patients, bleeding may not occur due to cervical stenosis. causing hematometra/pyometra.
Smt. Gupta presented with bleeding PV and enlarged inguinal nodes. She was diagnosed as a case of endometrial carcinoma. State the stage
| A |
Stage II |
|
| B |
Stage III |
|
| C |
Stage IV |
|
| D |
Stage I |
Smt. Gupta presented with bleeding PV and enlarged inguinal nodes. She was diagnosed as a case of endometrial carcinoma. State the stage
| A |
Stage II |
|
| B |
Stage III |
|
| C |
Stage IV |
|
| D |
Stage I |
Ans. is c i.e. Stage IV
Which of the following direct lymph node dissections in endometrial carcinoma :
| A |
Penetration into half of myometrium |
|
| B |
Clear cell Ca |
|
| C |
Fundal involvement |
|
| D |
All |
Which of the following direct lymph node dissections in endometrial carcinoma :
| A |
Penetration into half of myometrium |
|
| B |
Clear cell Ca |
|
| C |
Fundal involvement |
|
| D |
All |
Ans. is a, b and c i.e. Penetration into half of myometrium; Clear cell tumour; and Papillary serous carcinom
Indications for lymph node (Pelvic and Para-aortic) dissection in Endometrial cancer (also Indications of poor Prognosis).
1. Tumour histology :
- Clear cell carcinoma
- Papillary serous carcinoma
- Squamous carcinoma
- Adenocarcinoma (Endometriod) grade II and Ill.
- More than half of myometrial Invasion
- Isthmus- cervix extension
- Tumour size > 2cms
- Extrauterine disease.
As far as Peritoneal metastasis is concerned :
“Positive Peritoneal cytology in itself is not a marker of poor prognosis i.e. is not an indication for lymph node dissection unless and until associated with other poor prognostic markers as above.”
The most malignant endometrial carcinoma is :
| A |
Adenocarcinoma |
|
| B |
Adenoacanthoma |
|
| C |
Mixed adenosquamous carcinoma |
|
| D |
Clear cell carcinoma |
The most malignant endometrial carcinoma is :
| A |
Adenocarcinoma |
|
| B |
Adenoacanthoma |
|
| C |
Mixed adenosquamous carcinoma |
|
| D |
Clear cell carcinoma |
Ans. is d i.e. Clear cell carcinoma
Endometrial cancers can be histologically classified as :
Features Type I ‘Type II
Unopposed estrogen Present Absent
Menopausal status Pre-and perimenopausal Postmenopausal
Hyperplasia Present Balck
Race White Black
Grade Low High
Myometrial invasion Minimal Deep
Specific subtypes Endometrioid Serous, clear cell
Behavior Stable Aggressive
non ednometriod / type II endometrial cancer (clear cell carcinoma) have poor prognosis. Also know : Clear cell carcinoma :
- It accounts for < 5% of all endometrial carcinoma.
- The cells have highly atypical nuclei and abundant clear or eosinophilic cytoplasm.
- The cells have hobnail configuration.
- It characteristically occurs in older women and is very aggressive type of endometrial cancer.
- Prognosis is similar to or worse than papillary serous carcinoma.
Stage IV endometrial carcinoma, treatment is :
| A |
Surgery |
|
| B |
Radiotherapy |
|
| C |
Chemotherapy |
|
| D |
Radiotherapy, Chemotherapy and hormonal therapy |
Stage IV endometrial carcinoma, treatment is :
| A |
Surgery |
|
| B |
Radiotherapy |
|
| C |
Chemotherapy |
|
| D |
Radiotherapy, Chemotherapy and hormonal therapy |
Radiotherapy, Chemotherapy and hormonal therapy
All are risk factor for endometrial carcinoma except :
| A |
Diabetes |
|
| B |
Hypertension |
|
| C |
Obesity |
|
| D |
Multiparity |
All are risk factor for endometrial carcinoma except :
| A |
Diabetes |
|
| B |
Hypertension |
|
| C |
Obesity |
|
| D |
Multiparity |
Multiparity
Estrogen in the OCP causes all the following except :
| A |
Carcinoma in situ cervix |
|
| B |
Breast carcinoma |
|
| C |
Endometrial carcinoma |
|
| D |
Thromoembolism |
Estrogen in the OCP causes all the following except :
| A |
Carcinoma in situ cervix |
|
| B |
Breast carcinoma |
|
| C |
Endometrial carcinoma |
|
| D |
Thromoembolism |
Carcinoma in situ cervix
D and C is useful in the diagnosis of :
| A |
Genital TB |
|
| B |
Endometrial carcinoma |
|
| C |
DUB |
|
| D |
All |
D and C is useful in the diagnosis of :
| A |
Genital TB |
|
| B |
Endometrial carcinoma |
|
| C |
DUB |
|
| D |
All |
All
Most common cause of postmenopausal vaginal bleeding is?
| A | Endometrial carcinoma | |
| B |
Carcinoma cervix |
|
| C | Carcinoma vulva | |
| D |
Ovarian tumor |
Most common cause of postmenopausal vaginal bleeding is?
| A | Endometrial carcinoma | |
| B |
Carcinoma cervix |
|
| C | Carcinoma vulva | |
| D |
Ovarian tumor |
Endometrial carcinoma REF: Berek and Novak’s gynecology by Jonathan S. Berek, Emil Novak page 1349, Blueprints Obstetrics and Gynecology by Tamara L. Callahan, Aaron B. Caughey page 238
- “The most common cause of post-menopausal bleeding is endometrial and/or vaginal atrophy (not in options), not cancer. Endometrial cancer accounts for only 10-15% of cases”
- “However since endometrial malignancy can coexist with atrophic changes and with HRT, endometrial carcinoma must be ruled out in any case of post-menopausal bleeding”
- The most common malignancy to present with postmenopausal bleeding is Endometrial carcinoma
- The most common cause of post coital vaginal bleeding is cervical cancer.
Causes of post-menopausal bleeding:
|
Cause |
Percentage |
|
Endometrial atrophy |
60-80 |
|
Exogenous estrogen |
15-25 |
|
Endometrial cancer |
10 |
|
Endometrial polyps |
2-12 |
|
Endometrial hyperplasia |
5-10 |
The use of tamoxifen for breast cancer can cause all of the following adverse effects, except:
| A |
The use of tamoxifen for breast cancer can cause all of the following adverse effects, except: |
|
| B |
Endometrial carcinoma |
|
| C |
Carcinoma in contralateral breast |
|
| D |
Cataract |
The use of tamoxifen for breast cancer can cause all of the following adverse effects, except:
| A |
The use of tamoxifen for breast cancer can cause all of the following adverse effects, except: |
|
| B |
Endometrial carcinoma |
|
| C |
Carcinoma in contralateral breast |
|
| D |
Cataract |
Tamoxifen reduces the recurrence rate of breast cancer in ipsilateral as well as contralateral breasts.
Adverse effects associated with the use of tamoxifen are:
- 2-3 fold increased risk of thromboembolism
- 2-3 fold increased risk of endometrial carcinoma
- Hot flushes, vomiting, vaginal discharge, menstrual irregularities
- Cataract, dermatitis, depression, mild leucopenia
Treatment of choice of stage 1A grade 1 endometrial carcinoma is:
| A |
Radiotherapy |
|
| B |
Chemotherapy |
|
| C |
Chemotherapy plus radiotherapy |
|
| D |
None of the above |
Treatment of choice of stage 1A grade 1 endometrial carcinoma is:
| A |
Radiotherapy |
|
| B |
Chemotherapy |
|
| C |
Chemotherapy plus radiotherapy |
|
| D |
None of the above |
Patients with stage 1A grade I endometrial carcinoma, tumor is limited to the endometrium and is effectively managed by total abdominal hysterectomy with bilateral salphingo- oophorectomy.
Ref: Textbook of Obstetrics By D.C.Dutta, 6th Edition, Pages 329-334.
The risk of endometrial carcinoma is the highest with the following histological pattern of endometrial hyperplasia:
| A |
Simple hyperplasia without atypia |
|
| B |
Simple hyperplasia with atypia |
|
| C |
Complex hyperplasia without atypia |
|
| D |
Complex hyperplasia with atypia |
The risk of endometrial carcinoma is the highest with the following histological pattern of endometrial hyperplasia:
| A |
Simple hyperplasia without atypia |
|
| B |
Simple hyperplasia with atypia |
|
| C |
Complex hyperplasia without atypia |
|
| D |
Complex hyperplasia with atypia |
| A |
1, 2, 3 and 4 |
|
| B |
1, 3 and 4 |
|
| C |
2, 3 and 4 |
|
| D |
1 and 2 |
| A |
1, 2, 3 and 4 |
|
| B |
1, 3 and 4 |
|
| C |
2, 3 and 4 |
|
| D |
1 and 2 |
In Endometrial carcinoma, which of the following tumor suppressor gene occurs?
| A |
P53 |
|
| B |
Rb |
|
| C |
PTEN |
|
| D |
APC |
In Endometrial carcinoma, which of the following tumor suppressor gene occurs?
| A |
P53 |
|
| B |
Rb |
|
| C |
PTEN |
|
| D |
APC |
o PTEN is a tumor suppressor gene which is implicated in the causation of endometrial and prostate carcinoma.
Which is not a risk factor of endometrial carcinoma –
| A |
Obesity |
|
| B |
Smoking |
|
| C |
Infertility |
|
| D |
Tamoxifen |
Which is not a risk factor of endometrial carcinoma –
| A |
Obesity |
|
| B |
Smoking |
|
| C |
Infertility |
|
| D |
Tamoxifen |
Ans. is ‘b’ i.e., Smoking
Endometrial carcinoma
o Endometrial carcinoma is the most common invasive cancer of the female genital tract and accounts for 7% of all invasive cancer in women.
o The peak incidence is in the 55- to 65-year-old woman.
o Clinicopathological studies & molecular analysis support its classification into two major broad categories.
Type-I Carcinoma
o Most common type.
o Majority are well differentiated & mimic proliferative endometetrial glands.
o They are associated with- obesity, diabetes, hypertension, infertility and unopposed estrogen stimulation. Tamoxifen also increases the risk of endometrial cancer.
o Endometrial hyperplasia is a precursor to endometroid carcinoma.
o Mutation in PTEN tumor suppressor gene have been seen in 30-80% of endometeriod carcinoma & 20% patients with endometrial hyperplasia.
o Additional molecular changes that are common are microsatellite instability & mutations in KRAS & beta catenin oncogenes.
Type-H Carcinoma
o These occur in women a decade later than type I carcinoma.
o These usually arise in setting of endometrial atropy.
o They are poorly differentiated. The most common subtype is serous carcinoma, clear cell type & malignant mixed mullerian tumor.
o The most frequent alteration described is mutation in p53 tumor suppressor gene.
The risk of endometrial carcinoma is highest with the following histological pattern of endometrial hyperplasia:
March 2007
| A |
Simple hyperplasia with atypia |
|
| B |
Simple hyperplasia without atypia |
|
| C |
Complex hyperplasia with atypia |
|
| D |
Complex hyperplasia without atypia |
The risk of endometrial carcinoma is highest with the following histological pattern of endometrial hyperplasia:
March 2007
| A |
Simple hyperplasia with atypia |
|
| B |
Simple hyperplasia without atypia |
|
| C |
Complex hyperplasia with atypia |
|
| D |
Complex hyperplasia without atypia |
Ans. C: Complex hyperplasia with atypia
Simple hyperplasia progresses to cancer in 10-20% whereas atypical hyperplasia is a precursor of cancer in 60-70% of cases.
Classification
Most endometrial cancers are carcinomas (usually adenocarcinomas
Endometrial carcinomas can be classified into two pathogenetic groups:
- Type I: These cancers occur most commonly in pre- and peri-menopausal women, often with a history of unopposed estrogen exposure and/or endometrial hyperplasia. They are often minimally invasive into the underlying uterine wall, are of the low-grade endometrioid type, and carry a good prognosis.
- Type II: These cancers occur in older, post-menopausal women, and are not associated with increased exposure to estrogen. They are typically of the high-grade endometrioid, papillary serous or clear cell types, and carry a generally poor prognosis
Risk factors
- High levels of estrogen
- Endometrial hyperplasia
- Polycystic ovary syndrome
- Nulliparity
- Infertility
- Early menarche
- Late menopause
- Endometrial polyps or other benign growths of the uterine lining
- Tamoxifen
- Hyperplasia
- Pelvic radiation therapy
- Breast cancer
- Ovarian cancer
Clinical evaluation
- A Pap smear may be either normal or show abnormal cellular changes.
- Endometrial curettage is the traditional diagnostic method.
- If endometrial curettage does not yield sufficient diagnostic material, a dilation and curettage (D and C) is necessary for diagnosing the cancer.
- Endometrial biopsy or aspiration may assist the diagnosis.
- Transvaginal ultrasound to evaluate the endometrial thickness in women with postmenopausal
Pathology
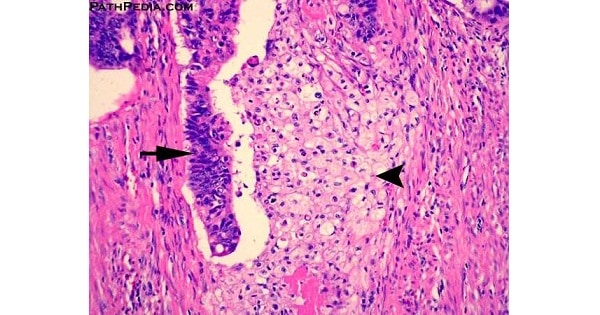
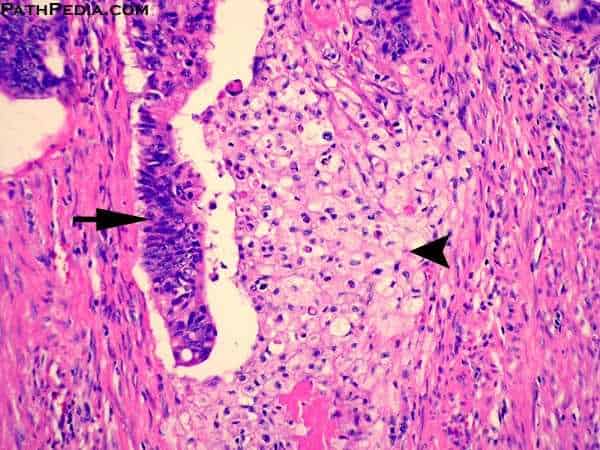
The most common finding is a well-differentiated endometrioid adenocarcinoma, which is composed of numerous, small, crowded glands with varying degrees of nuclear atypia, mitotic activity, and stratification.
Further evaluation
Colonoscopy is recommended due to the etiologic factors common to both endometrial cancer and colon cancer.
Staging
Endometrial carcinoma is surgically staged using the FIGO cancer staging system.
i a. Stage IA: tumor is limited to the endometrium
i b. Stage IB: invasion of less than half the myometrium
i c. Stage IC: invasion of more than half the myometrium
ii a. Stage IIA: endocervical glandular involvement only
ii b. Stage IIB: cervical stromal invasion
iii a.Stage IIIA: tumor invades serosa or adnexa, or malignant peritoneal cytology
iii b.Stage IIIB: vaginal metastasis
iii c. Stage IIIC: metastasis to pelvic or para-aortic lymph nodes
iv a. Stage IVA: invasion of the bladder or bowel
iv b.Stage IVB: distant metastasis, including intraabdominal or inguinal lymph nodes
Treatment
Abdominal hysterectomy is recommended over vaginal hysterectomy because it affords the opportunity to examine and obtain washings of the abdominal cavity to detect any further evidence of cancer.
Endometrial carcinoma with vaginal metastasis,what FIGO stage would it be :
September 2009
| A |
Stage III a |
|
| B |
Stage III b |
|
| C |
Stage III c |
|
| D |
Stage IV a |
Endometrial carcinoma with vaginal metastasis,what FIGO stage would it be :
September 2009
| A |
Stage III a |
|
| B |
Stage III b |
|
| C |
Stage III c |
|
| D |
Stage IV a |
Ans. B: Stage III b
The risk of endometrial carcinoma is highest with the following histological pattern .

| A |
Simple hyperplasia with atypia |
|
| B |
Simple hyperplasia without atypia |
|
| C |
Complex hyperplasia with atypia |
|
| D |
Complex hyperplasia without atypia |
The risk of endometrial carcinoma is highest with the following histological pattern .
| A |
Simple hyperplasia with atypia |
|
| B |
Simple hyperplasia without atypia |
|
| C |
Complex hyperplasia with atypia |
|
| D |
Complex hyperplasia without atypia |
This histological pattern is of endometrial hyperplasia
Ans. C: Complex hyperplasia with atypia
Simple hyperplasia progresses to cancer in 10-20% whereas atypical hyperplasia is a precursor of cancer in 60-70% of cases.
Classification
Most endometrial cancers are carcinomas (usually adenocarcinomas
Endometrial carcinomas can be classified into two pathogenetic groups:
- Type I: These cancers occur most commonly in pre- and peri-menopausal women, often with a history of unopposed estrogen exposure and/or endometrial hyperplasia. They are often minimally invasive into the underlying uterine wall, are of the low-grade endometrioid type, and carry a good prognosis.
- Type II: These cancers occur in older, post-menopausal women, and are not associated with increased exposure to estrogen. They are typically of the high-grade endometrioid, papillary serous or clear cell types, and carry a generally poor prognosi

