

Giardiasis
A mother brought her daughter with complaints of diarrhea. Lab investigations revealed Giardia lamblia. She had the same complaint before few weeks and was treated. She also had history of getting recurrent chest infections. This girl may have:
| A |
Severe combined immunodeficiency |
|
| B |
Common variable immunodeficiency |
|
| C |
Digeorge Syndrome |
|
| D |
C8 deficiency |
A mother brought her daughter with complaints of diarrhea. Lab investigations revealed Giardia lamblia. She had the same complaint before few weeks and was treated. She also had history of getting recurrent chest infections. This girl may have:
| A |
Severe combined immunodeficiency |
|
| B |
Common variable immunodeficiency |
|
| C |
Digeorge Syndrome |
|
| D |
C8 deficiency |
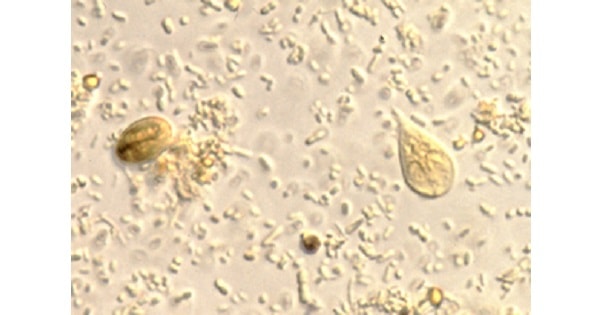
An anxious mother brought her 4 year old daughter to the pediatrician. The girl was passing loose bulky stools for the past 20 days. This was often associated with pain in abdomen. The pediatrician ordered the stool examination, which showed pear-shaped, flagellated trophozoites and cyst with four nuclei. What is the likely causative organism?
| A |
Entamoeba histolytica |
|
| B |
Giardia lamblia |
|
| C |
Cryptosporidium |
|
| D |
E.Coli |
An anxious mother brought her 4 year old daughter to the pediatrician. The girl was passing loose bulky stools for the past 20 days. This was often associated with pain in abdomen. The pediatrician ordered the stool examination, which showed pear-shaped, flagellated trophozoites and cyst with four nuclei. What is the likely causative organism?
| A |
Entamoeba histolytica |
|
| B |
Giardia lamblia |
|
| C |
Cryptosporidium |
|
| D |
E.Coli |
The typical morphology of the trophozoite and cyst of Giardia Lambia and the clinical picture make the diagnosis of Giardia Lamblia infection.
Prominent early symptoms include diarrhea, abdominal pain, bloating, belching, flatus, nausea, and vomiting. Although diarrhea is common, upper intestinal manifestations such as nausea, vomiting, bloating, and abdominal pain may predominate.
The duration of acute giardiasis is usually >1 week, although diarrhea often subsides.
Which of the following is/are diagnostic for giardia infection?
| A |
String test |
|
| B |
Serologic testing |
|
| C |
Finding trophozoites or cysts in the stool |
|
| D |
A and C |
Which of the following is/are diagnostic for giardia infection?
| A |
String test |
|
| B |
Serologic testing |
|
| C |
Finding trophozoites or cysts in the stool |
|
| D |
A and C |
The life cycle of giardia consists of two stages, the trophozoite and the cyst.
The trophozoite is pear-shaped with two nuclei, four pairs of flagella, and a suction disc with which it attaches to the intestinal wall.
The oval cyst is thick-walled with four nuclei and several internal fibers.
Each cyst gives rise to two trophozoites during excystation in the intestinal tract.
A man working in a constructing company presented with watery, foul-smelling diarrhea since 3 weeks. There is no blood in the stools. If it is giardiasis, it is best diagnosed by:
| A |
CFT |
|
| B |
Presence of both cysts and trophozoites in stools |
|
| C |
Presence of cysts only |
|
| D |
Haemagglutination |
A man working in a constructing company presented with watery, foul-smelling diarrhea since 3 weeks. There is no blood in the stools. If it is giardiasis, it is best diagnosed by:
| A |
CFT |
|
| B |
Presence of both cysts and trophozoites in stools |
|
| C |
Presence of cysts only |
|
| D |
Haemagglutination |
Which of the following substances in human milk is protective against Giardiasis?
| A |
Lactoferrin |
|
| B |
peroxidase |
|
| C |
Bile salt stimulated lipase |
|
| D |
PABA |
Which of the following substances in human milk is protective against Giardiasis?
| A |
Lactoferrin |
|
| B |
peroxidase |
|
| C |
Bile salt stimulated lipase |
|
| D |
PABA |
Giardia trophozoites in endoscopic study and biopsy of the duodenum is seen in:
| A |
Lactase deficiency |
|
| B |
Whipples disease |
|
| C |
Abetelipoprotenemia |
|
| D |
Immune globulin deficiency |
Giardia trophozoites in endoscopic study and biopsy of the duodenum is seen in:
| A |
Lactase deficiency |
|
| B |
Whipples disease |
|
| C |
Abetelipoprotenemia |
|
| D |
Immune globulin deficiency |
Biopsy of the small intestinal mucosa:
Giardiasis is associated with –
| A |
Common variable immunodeficiency |
|
| B |
C esterase deficiency |
|
| C |
C, deficiency |
|
| D |
Anaemia |
Giardiasis is associated with –
| A |
Common variable immunodeficiency |
|
| B |
C esterase deficiency |
|
| C |
C, deficiency |
|
| D |
Anaemia |
Ans. is ‘a’ i.e., Common variable immunodeficiency
Giardiasis is associated with
. Autosomal recessive agammaglobulinemia Common variable immune deficiency
. Selective IgA deficiency
. X-lined agammaglobulinemia
True about Giardia is –
| A |
May cause traveller’s diarrhoea |
|
| B |
Giardia inhabits ileum |
|
| C |
Trophozoites are infective to man |
|
| D |
None of the above |
True about Giardia is –
| A |
May cause traveller’s diarrhoea |
|
| B |
Giardia inhabits ileum |
|
| C |
Trophozoites are infective to man |
|
| D |
None of the above |
Ans. is ‘a’ i.e., May cause traveller’s diarrhoea
. Giardia can cause traveller’s diarrhea.
. Other protozoal causes of traveller’s diarrhea
– Entamoeba histolytica
– Cyclospora
– Cryptosporidium
. Giardia inhabits the proximal small intestine i..e, duodenum and upper jejunum (not ileum).
. The infective stage for giardial infection is cyst (not trophozoites).
A case of giardiasis presents with –
| A |
Nausea and vomiting |
|
| B |
Abdominal pain |
|
| C |
Steatorrhea and flatulence |
|
| D |
All of the above |
A case of giardiasis presents with –
| A |
Nausea and vomiting |
|
| B |
Abdominal pain |
|
| C |
Steatorrhea and flatulence |
|
| D |
All of the above |
Ans. is ‘d’ i.e., All of the above
Giardiasis
. Disease manifestations of giardiasis range from asymptomatic carriage to fulminant diarrhea and malabsorption.
. Most infected persons are asymptomatic
. The mechanisms by which Giardia causes alteration in small bowel function are largely unknown. Although trophozoites adhere to the epithelium, they do not cause invasive or locally destructive alterations.
. In most cases the morphology of the bowel is unaltered but in few cases; in chronically infected symptomatic patients; the histopathologic finding (flattened villi) and the clinical manifestations resemble those of tropical sprue and gluten sensitive enteropathy.
- Incubation period – I to 3 weeks
. Clinical manifestations
– Diarrhea – Nausea
– Abdominal pain – Vomiting
– Bloating – Flatus
– Extraintestinal – urticaria, anterior uveitis, arthritis.
. Fever, the presence of blood or mucus in the stools suggest a different diagnosis as all these are absent in giardiasis.
A patient presents with diarrhoea. analysis of stool on wet mount shows mobile protozoa without RBCs and pus cells. The diagnosis is –
| A |
Balantidium coil |
|
| B |
Giardiasis |
|
| C |
Trichomonas hominis |
|
| D |
Entamoeba histolytica |
A patient presents with diarrhoea. analysis of stool on wet mount shows mobile protozoa without RBCs and pus cells. The diagnosis is –
| A |
Balantidium coil |
|
| B |
Giardiasis |
|
| C |
Trichomonas hominis |
|
| D |
Entamoeba histolytica |
Ans. is ‘b’ i.e., Giardiasis
. Mobile protozoa with absence of RBC’s and pus cells in stools in a patient with diarrhoea suggests giardiasis.
. In balantidum cob and entomoeba histolytica infections, pus cells and RBC’s will be present in stools.
Trichomonas hominis is considered as non-pathogenic
Which of the following is true with Giardia lamblia‑
| A |
Malabsorption commonly seen |
|
| B |
Trophozoite forms is binucleate |
|
| C |
Diarrhea is seen |
|
| D |
b and c |
Which of the following is true with Giardia lamblia‑
| A |
Malabsorption commonly seen |
|
| B |
Trophozoite forms is binucleate |
|
| C |
Diarrhea is seen |
|
| D |
b and c |
Ans. is ‘b’ i.e., Trophozoite forms is binucleate; ‘c’ i.e., Diarrhea is seen
. Malabsorption is seen only in few cases, most patients are asymptomatic.
. Most common presentation is diarrhea with abdominal pain, nausea and vomiting.
. Trophozoite is bilateral, symmetrical and all organs of body are paired.
– 2 Axostyles – 4 pairs of flagella
– 2 Nuclei – 2 Sucking discs.
. The gold – standard for diagnosis of giardiasis is microscopic demonstration of the trophozoite, cyst or both in faeces.
. Duodenal aspirate or jejunal biopsy (not Jejunal wash fluid) may be required for diagnosis——— Harrison p. 1200. Remember
. Metronidazole and tinidazole are drug of choice for Giardia lambia.
Abdominal pain, fat malabsorption & frothy stools suggests –
| A |
Amoebiasis |
|
| B |
Bacillary dysentry |
|
| C |
Giardiasis |
|
| D |
All |
Abdominal pain, fat malabsorption & frothy stools suggests –
| A |
Amoebiasis |
|
| B |
Bacillary dysentry |
|
| C |
Giardiasis |
|
| D |
All |
Ans. is ‘c’ i.e., Giardiasis
. Abdominal pain, fat malabsorption and frothy stool can occur both in giardiasis and pancreatic enzyme deficiency (chronic pancreatitis).
- Amoebiasis and bacillary dysentry do not cause malabsorption.
Intractable diarrhoea in children is caused by all except-
| A |
Cystic fibrosis |
|
| B |
Giardiasis |
|
| C |
Secreting tumors |
|
| D |
Milk allergy |
Intractable diarrhoea in children is caused by all except-
| A |
Cystic fibrosis |
|
| B |
Giardiasis |
|
| C |
Secreting tumors |
|
| D |
Milk allergy |
Ans. is ‘b’ i.e., Giardiasis
Intractable diarrhea
o Intractable diarrhea is defined as, chronic or recurring diarrhea not obviously or early diagnosed as to etiology. o Chronic diarrhea is defined as diarrhea lasting > 4 weeks.
Intractable diarrhea is caused by ‑
o Cystic fibrosis o Congenital enterokinase & Trypsinogen deficiencies
o Bile duct atresia o Food protein sensitivity (Cow’s milk protein intolerance)
o Abetalipoproteinemia o Carbohydrate intolerance
o Secretory diarrhoea o Diarrhoea due to exocrine pancreas deficiency
Giardiasis causes infectious type of diarrhea which responses to antiprotozoal therapy.
Profuse watery diarrhea in an immuno compromised child is due to –
| A |
Cryptococcus |
|
| B |
Amoeba |
|
| C |
Giardia |
|
| D |
Lactose intolerance |
Profuse watery diarrhea in an immuno compromised child is due to –
| A |
Cryptococcus |
|
| B |
Amoeba |
|
| C |
Giardia |
|
| D |
Lactose intolerance |
Ans. is ‘c’ i.e., Giardia
Diarrhea in immunocompromised child (AIDS) include bacterial (salmonella, compylobacter) ,protozoal (giardiasis, cryptosporidium), and viral (CMV, HSV) causes.
Recurrent Giardiasis is associated with:
| A |
Severe combined immunodeficiency |
|
| B |
Common variable immunodeficiency |
|
| C |
Digeorge syndrome |
|
| D |
C8 deficiency |
Recurrent Giardiasis is associated with:
| A |
Severe combined immunodeficiency |
|
| B |
Common variable immunodeficiency |
|
| C |
Digeorge syndrome |
|
| D |
C8 deficiency |
Answer is B (Common variable immunodeficiency):
Common variable deficiency is associated with recurrent chronic intestinal giardiasis.
- Common variable immunodeficiency is characterized by deficient production of antibodies.
- They have normal no. of B lymphocytes but these B lymphocytes fail to mature into plasma cells.
- This results in hypogammaglobulinemia, with reduction in all classes of immunoglobulins but sometimes only IgG is reduced.
Which of the following infestations lead to malabsorption:
March 2011
| A |
Giardia lamblia |
|
| B |
Ascaris lumbricoides |
|
| C |
Necator americana |
|
| D |
Ancylostoma duodenale |
Which of the following infestations lead to malabsorption:
March 2011
| A |
Giardia lamblia |
|
| B |
Ascaris lumbricoides |
|
| C |
Necator americana |
|
| D |
Ancylostoma duodenale |
Ans. A: Giardia lamblia
The stool in giardial infestation is voluminous, foul smelling and contains large amount of mucus and fat but no blood. This is due to malabsorption since the parasites are coated on the mucosa, thus absorption suffers
Giardia lamblia/Giardia intestinalis/Lamblia intestinalis/Giardia duodenalis)
- It is a flagellated protozoan parasite that colonizes and reproduces in the small intestine, causing giardiasis.
- The giardia parasite attaches to the epithelium by a ventral adhesive disc, and reproduces via binary fission.
- Giardiasis does not spread via the bloodstream, nor does it spread to other parts of the gastro-intestinal tract, but remains confined to the lumen of the small intestine.
- Giardia trophozoites absorb their nutrients from the lumen of the small intestine, and are anaerobes.
- If the organism is split and stained, it has a very characteristic pattern that resembles a familiar “smilev face” symbol.
- Chief pathways of human infection include
– Ingestion of untreated sewage
– Contamination of natural waters also occurs in watersheds where intensive grazing occurs
- The life cycle begins with a noninfective cyst being excreted with the feces of an infected individual.
- The cyst is hardy, providing protection from various degrees of heat and cold, desiccation, and infection from other organisms.
- A distinguishing characteristic of the cyst is four nuclei and a retracted cytoplasm.
- Once ingested by a host, the trophozoite emerges to an active state of feeding and motility.
- After the feeding stage, the trophozoite undergoes asexual replication through longitudinal binary fission.
- The resulting trophozoites and cysts then pass through the digestive system in the faeces.
- While the trophozoites may be found in the faeces, only the cysts are capable of surviving outside of the host.
- Distinguishing features of the trophozoites are large karyosomes and lack of peripheral chromatin, giving the two nuclei a halo appearance.
- Cysts are distinguished by a retracted cytoplasm.
- This protozoan lacks mitochondriaColonization of the gut results in inflammation and villous atrophy, reducing the gut’s absorptive capability.
- Symptoms of infection include (in order of frequency) diarrhea, malaise, excessive gas (often flatulence or a foul or sulphuric-tasting belch, which has been known to be so nauseating in taste that it can cause the infected person to vomit), steatorrhoea (pale, foul smelling, greasy stools), epigastric pain, bloating, nausea, diminished interest in food, possible (but rare) vomiting which is often violent, and weight loss.
- Pus, mucus and blood are occasionally present in the stool.
- It usually causes “explosive diarrhea” and while unpleasant, is not fatal.
- People with recurring Giardia infections, particularly those with a lack ,of the Immunoglobulin A antibody, may develop chronic disease.
It is a cause of vitamin B12 deficiency, this a result of the problems caused within the intestinal absorption system
Giardiasis true is all except ‑
| A |
Diarrhea with steatosis |
|
| B |
Bloody diarrhea |
|
| C |
Metronidazole is the drug of choice |
|
| D |
Absent fever |
Giardiasis true is all except ‑
| A |
Diarrhea with steatosis |
|
| B |
Bloody diarrhea |
|
| C |
Metronidazole is the drug of choice |
|
| D |
Absent fever |
Ans. is ‘b’ i.e., Bloody diarrhea
Giardiasis
- Most of the infected pateints are asymptomatic.
- Giardia causes diarrhea and malabsorption. Malabsortion is due to loss of brush border enzyme activities, which cause fat malabsorption (steatorrhea) and vitamin deficiency.
- There may be abdominal pain, bloating, nausea & vomiting, flatulence and flatus.
- The mechanisms by which Giardia causes alteration in small bowel function are largely unknown. Although trophozoites adhere to the epithelium, they do not cause invasive or locally destructive alterations.
- Fever, the presence of blood or mucus in the stools suggest a different diagnosis as all these are absent in giardiasis.
- Giardia may also cause traveller’s diarrhea.
- Predisposing conditions to giardiasis are agammaglobulinemia, common variable immunodeficiency, and selective IgA-deficiency.
Diagnosis and treatment
- The gold – standard for diagnosis of giardiasis is microscopic demonstration of the trophozoite, cyst or both in faeces.
- Duodenal aspirate or jejunal biopsy may be required for diagnosis.
- In acute giardiasis trophozoites show the typical “falling-leaf” motility in wet mount examination of faeces. o Metronidazole and tinidazole are drug of choice for Giardia lambia.

