Hypothyroidism
All are seen in hypothyroidism except ‑
| A |
Weight gain |
|
| B |
Cold intolerance |
|
| C |
Diarrhoea |
|
| D |
Menorrhgia |
All are seen in hypothyroidism except ‑
| A |
Weight gain |
|
| B |
Cold intolerance |
|
| C |
Diarrhoea |
|
| D |
Menorrhgia |
Ans. is ‘c’ i.e., Diarrhea
Diarrhea is a feature of hyperthyroidism.
Hypothyroidism
o Iodine deficiency is the most common cause of hypothyroidism
o In area of iodine sufficiency, autoimmune thyroiditis (Hashimoto’s disease) is the most common cause.
|
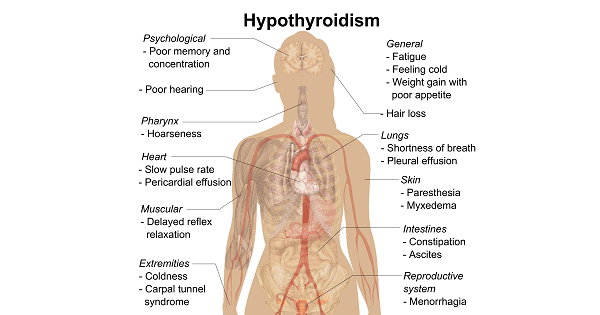
Clinical features of hypothyroidism
o Hoarseness of voice o Extreme somonlence |
o Menorrhgia, amenorrhea —> oligomenorrhea |
NOT a feature of hypothyroidism is ‑
| A |
Short metacarpals in hands |
|
| B |
Delayed puberty |
|
| C |
Delayed bone age |
|
| D |
Altered upper and lower segment ratio |
NOT a feature of hypothyroidism is ‑
| A |
Short metacarpals in hands |
|
| B |
Delayed puberty |
|
| C |
Delayed bone age |
|
| D |
Altered upper and lower segment ratio |
Ans. is ‘a’ i.e., Short metacarpal in hands
Hypothyroidism
o Hypothyroidism results from deficient production of thyroid hormone or a defect in thyroid hormone receptor activity.
o Hypothyroidism may be : –
i) Congenital —> Present since birth
ii) Acquired –> Symptoms appear after a period of apparently normal thyroid function.
Hypothyroidism causes –
i) Delayed bone growth (Bone age markedly delayed)
ii) Delayed puberty &
Alteration in upper and lower segment ratio (upper segment > lower segment)
Hypothyroidism
o Hypothyroidism results from deficient production of thyroid hormone or a defect in thyroid hormone receptor activity.
o Hypothyroidism may be : –
i) Congenital —> Present since birth
ii) Acquired –> Symptoms appear after a period of apparently normal thyroid function.
Hypothyroidism causes –
i) Delayed bone growth (Bone age markedly delayed)
ii) Delayed puberty &
Alteration in upper and lower segment ratio (upper segment > lower segment)
Hypothyroidism may be caused by
| A |
Lithium |
|
| B |
Hematochromatosis |
|
| C |
Scleroderma |
|
| D |
All of the above |
Hypothyroidism may be caused by
| A |
Lithium |
|
| B |
Hematochromatosis |
|
| C |
Scleroderma |
|
| D |
All of the above |
Answer is D (All of the above):
Hypothyroidism may be caused by drugs like Lithium and /or Infiltrative disorders like Scleroderma and Hematochromatosis.
Causes of Hypothyroidism
|
Causes of Hy pothyroidism |
|
|
Primary |
|
|
• |
Autoimmune hypothyroidism: Hoshimoto’s thyroiditis, atrophic thyroiditis |
|
• |
Iatrogenic: 1311treatment, subtotal or total thyroidectomy, external irradiation of neck for lymphoma or cancer |
|
• |
Drugs: Iodine excess (including iodine-containing contrast media and amiodarone), lithium, antithyroid drugs, p-aminosalicylic acid, interferon-a and other cytokines, aminoglutethimide |
|
• |
Congenital hypothyroidism: absent or ectopic thyroid gland, dyshormogenesis, TSH-R mutation |
|
• |
Iodine deficiency |
|
• |
Infiltrative disorders: amyloidosis, sarcoidosis, hemochromatosis, scleroderma, cystinosis, Riedel’s thyroiditis |
|
• |
Overexpression of type 3 deoiodinase in infantile hemangioma |
|
Transient |
|
|
• |
Silent thyroiditis, including postpartum thyroiditis |
|
• |
Subacute thyroiditis |
|
• |
Withdrawal of thyroxine treatment in individuals with an intact thyroid |
|
• |
After 1311 treatment or subtotal thyroidectomy for Grave’s disease |
|
Secondary |
|
|
• |
Hypopituitarism: tumors, pituitary surgery or irradiation, infiltrative disorders, Sheehan’s syndrome, trauma, genetic forms of combined pituitary hormone deficiencies |
|
• |
Isolated TSH deficiency or inactivity |
|
• |
Bexarotene treatment |
|
• |
Hypothalamic disease: tumors, trauma, infiltrative disorders, idiopathic |
TSH, thyroid-stimulating hormone; TSH-R, TSH receptor.

Hypothyroidism in sub-himlayan region is due to deficiency of
| A |
Iron |
|
| B |
Iodine |
|
| C |
Copper |
|
| D |
Selenium |
Hypothyroidism in sub-himlayan region is due to deficiency of
| A |
Iron |
|
| B |
Iodine |
|
| C |
Copper |
|
| D |
Selenium |
Answer is B (Iodine):
Hypothyroidism (and Endemic Goitre) in sub-himalayan region is primarily due to deficiency of iodine.
‘Dietary iodine deficiency is widely prevalent in many parts of India, especially the sub-Himalayan region and is the principal cause of endemic goiter. Where the deficiency is severe, goiter, hypothyroidism and endemic cretinism is common’-‘Pediatrics: A concise Test’ by kabra Elsevier 2007/2
The most common cause of neonatal hypothyroidism (congenital hypothyroidism) is thyroid gland dysgenesis (80-85%).
The most common of endemic goiter/hypothyroidism is iodine deficiency.
Which of the following is associated with hypothyroidism in Himalayan region?
| A |
Cu |
|
| B |
Fe |
|
| C |
Zn |
|
| D |
Selenium |
Which of the following is associated with hypothyroidism in Himalayan region?
| A |
Cu |
|
| B |
Fe |
|
| C |
Zn |
|
| D |
Selenium |
Answer is D (Selenium): Hypothyroidism and Hashimoto’s Thyroiditis (2013)
Hypothyroidism in Himalayan region is associated with Iodine Deficiency and Selenium deficiency.
Selenium is a trace element that plays a role in thyroid hormone production, as it forms part of a seleno-enzyme responsible for converting T4 into T3. Selenium deficiency as a causative factor for Hypothyroidism and Goitre formation has been explained by diminished activity of selenocysteine enzymes in thyroid, notably glutathione peroxidase and deiodinase type-1. Type-1 deiodinase enzyme is required for conversion of T4 to T3 in peripheral tissues. Mountainous regions, such as the Himalayas, the Andes, and the Alps, and flooded river valleys, such as the Ganges, are among the most severely iodine-deficient areas in the world. The problem of Iodine deficiency in these areas is further compounded by deficiency of Selenium.
Which of the following is not associated with hypothyroidism
| A |
Low T3 |
|
| B |
High TSH |
|
| C |
High Triglycerides |
|
| D |
Low cholesterol |
Which of the following is not associated with hypothyroidism
| A |
Low T3 |
|
| B |
High TSH |
|
| C |
High Triglycerides |
|
| D |
Low cholesterol |
Answer is D (Low cholesterol):
Hypothyroidism is associated with increased cholesterol (Hypercholesterolemia) and not with low cholesterol (Hypocholesterolemia).
A normal TSH excludes primary (but not secondary) hypothyroidism. If the TSH is elevated an unbound T4 level is needed to confirm the presence of clinical hypothyroidism but T4 is inferior to TSH where used as a screening test.
*Circulating unbound T3 (Free T3) levels may be normal in about 25% of patients reflecting adaptive diodinase responses to hypothyroidism. Free T3 measurements are therefore not indicated.
Yellowing of the skin occurs in hypothyroidism because of:
| A |
Increased bilirubin |
|
| B |
Increased cholesterol |
|
| C |
Increased carotene |
|
| D |
Increased |
Yellowing of the skin occurs in hypothyroidism because of:
| A |
Increased bilirubin |
|
| B |
Increased cholesterol |
|
| C |
Increased carotene |
|
| D |
Increased |
Answer is C (Increased Carotene):
The yellow colour of skin in patients with hypothyroidism results from the accumulation of carotene (carotenoderma) in the top layer of the epidermis (Stratum Corneum). Increased levels of carotene are believed to result from impaired hepatic conversion of beta-carotene to Vitamin A.
7′4 is essential for conversion of carotene to vitamin A. In hypothyroidism, this reaction is very slow and carotene accumulation in the blood and tissue (carotenaemia) gives a yellow colour to the skin (carotenoderma). Carotenaemia can be clinically differentiated from jaundice by the fact that sclera of the eyeballs are not affected Carotenaemia
All of the following are features of hypothyroidism except:
September 2005
| A |
Dry skin |
|
| B |
Bradycardia |
|
| C |
Myxedema |
|
| D |
Lid retraction |
All of the following are features of hypothyroidism except:
September 2005
| A |
Dry skin |
|
| B |
Bradycardia |
|
| C |
Myxedema |
|
| D |
Lid retraction |
Ans. D: Lid retraction
Common features of hypothyroidism include easy fatigability, coldness, weight gain, constipation, menstrual irregularities, and muscle cramps.
Physical findings include a cool, rough, dry skin, puffy face and hands (myxedema),hair becomes dry and tends to fall, a hoarse, husky voice, and slow reflexes.
A – Cardiovascular Signs
Impaired muscular contraction, bradycardia, and diminished cardiac output. Cardiac enlargement may occur, due in part to interstitial edema, nonspecific myofibrillary swelling, and left ventricular dilatation but often to pericardial effusion. Although cardiac output is reduced, congestive heart failure and pulmonary edema are rarely noted.
B – Pulmonary Function
Shallow, slow respiration and impaired respiratory response to hypercapnia or hypoxia. Respiratory failure is a major problem in patients with myxedema coma.
C – Gastrointestinal Tract
Peristalsis is markedly slowed, resulting in chronic constipation and occasionally severe fecal impaction or ileus.
D – Hematologic
Anemia is the major manifestation.
E – Renal Function
Decreased glomerular filtration rate and impaired ability to excrete water load.
F – Neuromuscular System
Severe muscle cramps, paresthesias, and muscle weakness.
G – Nervous System
Symptoms may include chronic fatigue, lethargy, and inability to concentrate.Carpal tunnel syndrome may occur. If untreated, hypothyroidism may pass into a hypothermic, stuporous state (myxedema coma) that may be fatal. Lid retraction is a manifestation of hyperthyroidism.
Not true about congenital hypothyroidism:
March 2009
| A |
Males more often affected |
|
| B |
No signs at birth |
|
| C |
Occurs due to antibodies against thyroid peroxisomes |
|
| D |
Seen in 1:4000 live births |
Not true about congenital hypothyroidism:
March 2009
| A |
Males more often affected |
|
| B |
No signs at birth |
|
| C |
Occurs due to antibodies against thyroid peroxisomes |
|
| D |
Seen in 1:4000 live births |
Ans. A: Males more often affected
Congenital Hypothyroidism (CH) is one of the most common preventable causes of mental retardation with a worldwide incidence of 1:4000 live births.
It is usually sporadic with a 2:1 female to male preponderance.
Thyroid dysgenesis is the commonest cause of permanent CH (80-85%).
Thyroid hormone synthetic defects account for 10% of all cases. These are inherited as autosomal recessive disorders. The defect can lie in iodide trapping or organification, iodotyrosine coupling or deiodination and thyroglobulin synthesis or secretion. The commonest of these is a defect in the thyroid peroxidase (TPO) activity leading to impaired oxidation and organification of iodide to iodine. These disorders usually result in goitrous hypothyroidism.
Majority of infants appear normal at birth.
Ideally universal screening at 3-4 days of age should be done for detecting CH.
Abnormal values on screening (T4 < 6.5 ug/dL, TSH >20mu/L) should be confirmed by a venous sample before initiating treatment.
Term as well as preterm infants with low T4 and elevated TSH should be started on L-thyroxine at a dose of 10-15ig/ kg/ day as soon as the diagnosis is made.
Regular monitoring should be done to ensure that T4 is in the upper half of normal range. The outcome of CH depends on the time of initiation of therapy and the dose of L-thyroxine used’
Most common cause of hypothyroidism in India:
September 2009
| A |
latrogenic |
|
| B |
Pituitary tumours |
|
| C |
Iodine deficiency |
|
| D |
Hashimoto’s disease |
Most common cause of hypothyroidism in India:
September 2009
| A |
latrogenic |
|
| B |
Pituitary tumours |
|
| C |
Iodine deficiency |
|
| D |
Hashimoto’s disease |
Ans. C: Iodine deficiency
Causes of hypothyroidism
- Iodine deficiency, the most common cause of hypothyroidism in India.
- Hashimoto’s disease, an autoimmune disorder.
- Iatrogenic (treatment of hyperthyroidism)
- Pregnancy-related condition, this hypothyroidism is usually temporary and often doesn’t require treatment.
- Radiation therapy done to head and neck
- Viral fever
- Pituitary tumours
- Genetic causes
- Certain drugs such as lithium for psychiatric ailments and amiodarone, a heart drug can lead to hypothyroidism
The commonest cause of congenital hypothyroidism:
September 2012
| A |
Thyroid dysgenesis |
|
| B |
Pendred syndrome |
|
| C |
Defective iodine release |
|
| D |
Deficiency of de-iodinase |
The commonest cause of congenital hypothyroidism:
September 2012
| A |
Thyroid dysgenesis |
|
| B |
Pendred syndrome |
|
| C |
Defective iodine release |
|
| D |
Deficiency of de-iodinase |
Ans. A i.e. Thyroid dysgenesis
Congenital hypothyroidism
- Large & open posterior fontanelle,
- Absent social smile & eyebrows,
- Growth retardation,
- Delayed puberty,
- Cold extremities,
- Large tongue,
- Prolongation of physiological jaundice &
- Epiphyseal dysgenesis
Which of the following antitubercular drugs is associated with hypothyroidism?
| A |
Rifampicin |
|
| B |
Pyrazinamide |
|
| C |
Ethionamide |
|
| D |
Streptomycin |
Which of the following antitubercular drugs is associated with hypothyroidism?
| A |
Rifampicin |
|
| B |
Pyrazinamide |
|
| C |
Ethionamide |
|
| D |
Streptomycin |
Ans. c. Ethionamide
