Laryngeal Paralysis
Cadaveric position of vocal cords is seen in
| A |
Bilateral recurrent and superior laryngeal nerve palsy |
|
| B |
Bilateral recurrent laryngeal nerve palsy |
|
| C |
Unilateral superior laryngeal nerve palsy |
|
| D |
Bilateral superior laryngeal nerve palsy |
Cadaveric position of vocal cords is seen in
| A |
Bilateral recurrent and superior laryngeal nerve palsy |
|
| B |
Bilateral recurrent laryngeal nerve palsy |
|
| C |
Unilateral superior laryngeal nerve palsy |
|
| D |
Bilateral superior laryngeal nerve palsy |
|
Position of cord |
Location from midline |
Defect |
|
Median |
midline |
RLN palsy |
|
Paramedian |
1.5 mm |
RLN palsy |
|
Intermediate |
3.5 mm |
Both RLN and superior laryngeal nerve palsy |
|
Gentle abduction |
7.5mm |
ADDUCTOR PALSY |
Bilateral recurrent laryngeal nerve palsy is seen in:
| A |
Thyroidectomy |
|
| B |
Carcinoma thyroid |
|
| C |
Cancer cervical oesophagus |
|
| D |
All of the above |
Bilateral recurrent laryngeal nerve palsy is seen in:
| A |
Thyroidectomy |
|
| B |
Carcinoma thyroid |
|
| C |
Cancer cervical oesophagus |
|
| D |
All of the above |
Complications of Hemithyroidectomy include all of the following, except?
| A |
Hypocalcemia |
|
| B |
Wound hematoma |
|
| C |
Recurrent laryngeal nerve palsy |
|
| D |
External branch of superior laryngeal nerve palsy |
Complications of Hemithyroidectomy include all of the following, except?
| A |
Hypocalcemia |
|
| B |
Wound hematoma |
|
| C |
Recurrent laryngeal nerve palsy |
|
| D |
External branch of superior laryngeal nerve palsy |
Hypocalcemia following total or subtotal thyroidectomy where all four parathyroid glands are either removed results due to parathyroid insufficiency.
Parathyroid insufficiency (hypocalcemia) is usually not seen after Hemithyroidectomy as it involves the removal of only one lobe of thyroid together with the isthmus and the parathyroids are preserved.
In complete bilateral palsy of recurrent laryngeal nerves, there is:
| A |
Complete loss of speech with stridor and dyspnea |
|
| B |
Complete loss of speech but no difficulty in breathing |
|
| C |
Preservation of speech with severe stridor and dyspnea |
|
| D |
Preservation of speech and no difficulty in breathing |
In complete bilateral palsy of recurrent laryngeal nerves, there is:
| A |
Complete loss of speech with stridor and dyspnea |
|
| B |
Complete loss of speech but no difficulty in breathing |
|
| C |
Preservation of speech with severe stridor and dyspnea |
|
| D |
Preservation of speech and no difficulty in breathing |
In patients having bilateral paralysis of recurrent laryngeal nerve, the airway is inadequate since both the cords lie in the median and paramedian position causing dyspnoea and stridor but the voice is preserved.
Cadaveric position of vocal cords is seen in:
| A |
Bilateral recurrent and superior laryngeal nerve palsy |
|
| B |
Bilateral recurrent laryngeal nerve palsy |
|
| C |
Unilateral superior laryngeal nerve palsy |
|
| D |
Bilateral superior laryngeal nerve palsy |
Cadaveric position of vocal cords is seen in:
| A |
Bilateral recurrent and superior laryngeal nerve palsy |
|
| B |
Bilateral recurrent laryngeal nerve palsy |
|
| C |
Unilateral superior laryngeal nerve palsy |
|
| D |
Bilateral superior laryngeal nerve palsy |
In bilateral recurrent and superior laryngeal nerve palsy all the laryngeal muscles are paralysed and both cords lie in the cadaveric position i.e 3.5mm from the midline. There is also total anaesthesia of the larynx.
- In bilateral recurrent laryngeal nerve palsy, vocal cords lie in median or paramedian position due to unapposed action of cricothyroid muscles.
- In unilateral paralysis of superior laryngeal nerve, there is shortening of the cord with loss of tension. The paralysed cord appears wavy due to lack of tension.
Twenty-four hours following partial thyroidectomy where the inferior thyroid artery was also ligated (tied off), the patient now spoke with a hoarse voice (whisper), and had difficulty in breathing. Which nerve was injured?
| A |
Internal branch of superior laryngeal |
|
| B |
Ansa cervicalis |
|
| C |
Ansa subclavia |
|
| D |
Recurrent laryngeal |
Twenty-four hours following partial thyroidectomy where the inferior thyroid artery was also ligated (tied off), the patient now spoke with a hoarse voice (whisper), and had difficulty in breathing. Which nerve was injured?
| A |
Internal branch of superior laryngeal |
|
| B |
Ansa cervicalis |
|
| C |
Ansa subclavia |
|
| D |
Recurrent laryngeal |
Injury of which of these nerve most commonly leads to vocal cord paralysis?
| A |
Recurrent laryngeal |
|
| B |
External laryngeal |
|
| C |
Internal laryngeal |
|
| D |
Superior laryngeal |
Injury of which of these nerve most commonly leads to vocal cord paralysis?
| A |
Recurrent laryngeal |
|
| B |
External laryngeal |
|
| C |
Internal laryngeal |
|
| D |
Superior laryngeal |
Recurrent laryngeal nerve injury is the most common cause of vocal cord paralysis. It from the Vagus, travels further on the left where it loops around the arch of Aorta while on the right, it travels around the subclavian artery. Supplies all the muscles (posterior Cricoarytenoid, interarytenoid, lateral Cricoarytenoid, and Thyroarytenoid muscles) except for Cricothyroid.
- Brainstem Nuclei
- Corticobulbar fibers start from the cerebral cortex and descend through the internal capsule and synapse at the nucleus ambiguus in the Medulla
- Vagus Nerve
- Recurrent Laryngeal Nerve is the commonest cause.
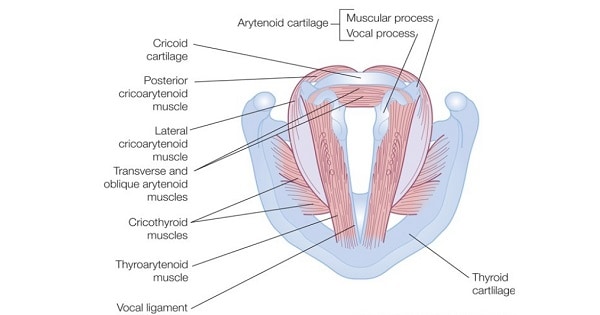
1. Posterior cricoarytenoid the ONLY abductor of the vocal folds. Functions to open the glottis by rotary motion on the arytenoid cartilages. Also tenses cords during phonation.
2. Lateral cricoarytenoid functions to close glottis by rotating arytenoids medially.
3. Transverse arytenoid only unpaired muscle of the larynx. Functions to approximate bodies of arytenoids closing posterior aspect of glottis.
4. Oblique arytenoid this muscle plus action of transverse arytenoid function to close laryngeal introitus during swallowing.
5. Thyroarytenoid – very broad muscle, usually divided into three parts:
- Thyroarytenoideus internus (vocalis) – adductor and major tensor of free edge of vocal fold.
- Thyroarytenoideus externus – major adductor of vocal fold
- Thyroepiglotticus – shortens vocal ligaments
Damage to the internal laryngeal nerve results in
| A |
Hoarseness |
|
| B |
Loss of timbre of voice |
|
| C |
Anaesthesia of the larynx |
|
| D |
Brathing difficulty |
Damage to the internal laryngeal nerve results in
| A |
Hoarseness |
|
| B |
Loss of timbre of voice |
|
| C |
Anaesthesia of the larynx |
|
| D |
Brathing difficulty |
Anesthesia of larynx
Thyroid Ca causes laryngeal paralysis due to
| A |
Recurrent laryngeal nerve palsy |
|
| B |
Vagus nerve palsy |
|
| C |
Glossopharyngeal nerve palsy |
|
| D |
Hypoglossal nerve palsy |
Thyroid Ca causes laryngeal paralysis due to
| A |
Recurrent laryngeal nerve palsy |
|
| B |
Vagus nerve palsy |
|
| C |
Glossopharyngeal nerve palsy |
|
| D |
Hypoglossal nerve palsy |
Ans. is ‘a’ i.e. Recurrent laryngeal nerve palsy
The nerves found in close relationship to thyroid gland and therefore likely to be involved in malignant spread and thyroid surgery are – recurrent laryngeal nerve and – superior laryngeal nerve.
Complications of Hemithyroidectomy include all of the following Except?
| A |
Hypocalcemia |
|
| B |
Wound hematoma |
|
| C |
Recurrent laryngeal nerve palsy |
|
| D |
External branch of superior laryngeal nerve palsy |
Complications of Hemithyroidectomy include all of the following Except?
| A |
Hypocalcemia |
|
| B |
Wound hematoma |
|
| C |
Recurrent laryngeal nerve palsy |
|
| D |
External branch of superior laryngeal nerve palsy |
Ans. is ‘a’ i.e. Hypocalcemia
“Transient or permanent hypocalcemia is very unlikely after hemithyroidectomy, since the opposite lobe is not
disturbed.”- Endocrine surgery by Arthur E. Schwartz
Hypocalcemia is seen after total or subtotal thyroidectomy d/t inadvertent removal of parathyroid glands or their injury during surgery.
After thyroidectomy, pt. developed stridor within 2 hrs. All are likely cause of stridor except :
| A |
Hypocalcemia |
|
| B |
Recurrent laryngeal nerve palsy |
|
| C |
Laryngomalacia |
|
| D |
Wound hematoma |
After thyroidectomy, pt. developed stridor within 2 hrs. All are likely cause of stridor except :
| A |
Hypocalcemia |
|
| B |
Recurrent laryngeal nerve palsy |
|
| C |
Laryngomalacia |
|
| D |
Wound hematoma |
Ans. is ‘a’ i.e. hypocalcemia
- Though hypocalcemia can cause stridor d/t laryngeal spasm, it is seen 2-5 days after operation. Bailey and Love write -“Most cases present dramatically 2-5 days after operation but, very rarely, the onset is delayed for 2-3 weeks or a patient with marked hypocalcemia is asymptomatic.”
- One shoudn’t be confused with laryngomalacia. This is not congenital laryngomalacia which occurs in the newborn. This laryngomalacia is softening of the larynx and trachea due to continuous pressure on it by a large goitre. Removal of the goitre causes collapse and kinking of the larynx and trachea leading to airway obstruction.
Which of the following will not lead to respiratory distress after Thyroid Surgery –
| A |
Laryngomalacia |
|
| B |
Bilateral recurrent laryngeal nerve injury |
|
| C |
Hypocalcemia |
|
| D |
None |
Which of the following will not lead to respiratory distress after Thyroid Surgery –
| A |
Laryngomalacia |
|
| B |
Bilateral recurrent laryngeal nerve injury |
|
| C |
Hypocalcemia |
|
| D |
None |
Ans is None
- All the given conditions are able to cause resp. distress.
- Endocrine surgery of Head & Neck writes
- “The reason for airway compromise include :
bilateral recurrent laryngeal nerve injury
tracheal malacia from longstanding tracheal compression caused by a large thyroid mass
subglottic edema from laryngeal involvement with tumor,
tracheal invasion by tumor
post-op hemorrhage or hematoma.”
Hypocalcemia can also cause stridor by causing laryngeal spasm
Vocal cord palsy in thyroid surgery is due to injury to‑
| A |
Superficial laryngeal nerve |
|
| B |
Recurrent laryngeal nerve |
|
| C |
Ansa cervicalis |
|
| D |
Vagus nerve |
Vocal cord palsy in thyroid surgery is due to injury to‑
| A |
Superficial laryngeal nerve |
|
| B |
Recurrent laryngeal nerve |
|
| C |
Ansa cervicalis |
|
| D |
Vagus nerve |
Ans. is ‘b’ i.e., Recurrent laryngeal nerve
Hoarseness secondary to bronchogenic carcinoma is usually due to extension of the tumour into ‑
| A |
Vocal cord |
|
| B |
Superior laryngeal nerve |
|
| C |
Left recurrent laryngeal nerve |
|
| D |
Right vagus nerve |
Hoarseness secondary to bronchogenic carcinoma is usually due to extension of the tumour into ‑
| A |
Vocal cord |
|
| B |
Superior laryngeal nerve |
|
| C |
Left recurrent laryngeal nerve |
|
| D |
Right vagus nerve |
Ans. is ‘c’ i.e., Left recurrent laryngeal nerve
A patient met with recurrent laryngeal nerve palsy while undergoing thyroid surgery. Which of the following muscles of larynx is/are affected?
| A |
Posterior crioarytenoid |
|
| B |
Lateral cricoarytenoid |
|
| C |
Thyroarytenoid |
|
| D |
All |
A patient met with recurrent laryngeal nerve palsy while undergoing thyroid surgery. Which of the following muscles of larynx is/are affected?
| A |
Posterior crioarytenoid |
|
| B |
Lateral cricoarytenoid |
|
| C |
Thyroarytenoid |
|
| D |
All |
All muscles which move the vocal cord (abductors, adductors or tensors) are supplied by the recurrent laryngeal nerve except the cricothyroid muscle which is supplied by external laryngeal nerve (a branch of superior laryngeal nerve).
Right sided vocal cord palsy seen in:
| A |
Larynx carcinoma |
|
| B |
Aortic aneurysm |
|
| C |
Mediastinal lymphadenopathy |
|
| D |
Right vocal nodule |
Right sided vocal cord palsy seen in:
| A |
Larynx carcinoma |
|
| B |
Aortic aneurysm |
|
| C |
Mediastinal lymphadenopathy |
|
| D |
Right vocal nodule |
- Lt RLN.: Arises from vagus in the mediastinum at the level of arch of aorta loops around it and then ascends into the neck.
- Rt. RLN: Arises from vagus at the level of subclavian artery, hooks around it and then ascends up.
So, any mediastinal causes viz mediastinal lymphadenopathy and aortic aneurysm would parlyse Lt. RLN. only
Vocal nodule does not cause vocal cord palsy.
Laryngeal carcinoma especially glottic can cause U/L or B/L Vocal Cord paralysis – Conn’s Current Theory
Bilateral (B/I) recurrent laryngeal nerve palsy is/ are caused by:
| A |
Thyroid surgery |
|
| B |
Thyroid malignancy |
|
| C |
Aneurysm of arch of aorta |
|
| D |
a and b |
Bilateral (B/I) recurrent laryngeal nerve palsy is/ are caused by:
| A |
Thyroid surgery |
|
| B |
Thyroid malignancy |
|
| C |
Aneurysm of arch of aorta |
|
| D |
a and b |
Cause of B/L Recurrent laryngeal nerve palsy is/are:
| A |
Thyroid Ca |
|
| B |
Thyroid Surgery |
|
| C |
Bronchogenic Ca |
|
| D |
a and b |
Cause of B/L Recurrent laryngeal nerve palsy is/are:
| A |
Thyroid Ca |
|
| B |
Thyroid Surgery |
|
| C |
Bronchogenic Ca |
|
| D |
a and b |
Bilateral recurrent laryngeal nerve palsy is seen in:
| A |
Thyroidectomy |
|
| B |
Carcinoma thyroid |
|
| C |
Cancer cervical oesophagus |
|
| D |
All of the above |
Bilateral recurrent laryngeal nerve palsy is seen in:
| A |
Thyroidectomy |
|
| B |
Carcinoma thyroid |
|
| C |
Cancer cervical oesophagus |
|
| D |
All of the above |
Causes of bilateral recurrent laryngeal nerve palsy are:
- Idiopathic
- Post thyroid surgery
- Thyroid malignancy
- Carcinoma of cervical part of esophagus
- Cervical Lymphadenopathy
Peripheral neuritis causes high vagal palsy which leads to both superior as well as recurrent laryngeal nerve palsy i.e. bilateral complete palsy.
Most common cause of B/L recurrent laryngeal paralysis:
| A |
Thyroid surgery |
|
| B |
Cancer cervical oesophagus |
|
| C |
Blow from nasal cavity |
|
| D |
Thyroid cancer |
Most common cause of B/L recurrent laryngeal paralysis:
| A |
Thyroid surgery |
|
| B |
Cancer cervical oesophagus |
|
| C |
Blow from nasal cavity |
|
| D |
Thyroid cancer |
Which one of the following lesions of vocal cord is dangerous to life:
| A |
Bilateral adductor paralysis |
|
| B |
Bilateral abductor paralysis |
|
| C |
Combined paralysis of left side superior and recurrent laryngeal nerve |
|
| D |
Superior laryngeal nerve paralysis |
Which one of the following lesions of vocal cord is dangerous to life:
| A |
Bilateral adductor paralysis |
|
| B |
Bilateral abductor paralysis |
|
| C |
Combined paralysis of left side superior and recurrent laryngeal nerve |
|
| D |
Superior laryngeal nerve paralysis |
Ans. is b i.e. bilateral abductor paralysis
- Most dangerous lesion of vocal cords is bilateral abductor paralysis (Bilateral RLN palsy).
- This is because recurrent laryngeal nerve palsy will lead to paralysis of all laryngeal muscles except the cricothyroid muscle (as it is supplied by superior laryngeal nerve). The cricothyroid muscle is an adductor & therefore this will leave both the cords in median or paramedian position thus endangering proper airway, leading to stridor and dyspnoea.
In complete bilateral palsy of recurrent laryngeal nerves, there is:
| A |
Complete loss of speech with stridor and dyspnea |
|
| B |
Complete loss of speech but not difficulty in breathing |
|
| C |
Preservation of speech with severe stridor and dyspnea |
|
| D |
Preservation of speech and not difficulty in breathin |
In complete bilateral palsy of recurrent laryngeal nerves, there is:
| A |
Complete loss of speech with stridor and dyspnea |
|
| B |
Complete loss of speech but not difficulty in breathing |
|
| C |
Preservation of speech with severe stridor and dyspnea |
|
| D |
Preservation of speech and not difficulty in breathin |
Ans. is c i.e. Preservation of speech with severe stridor and dyspnea
The voice in a patient with bilateral abductor paralysis of larynx is:
| A |
Puberuophonia |
|
| B |
Phonasthenia |
|
| C |
Dysphonia plicae ventricularis |
|
| D |
Normal or good voice |
The voice in a patient with bilateral abductor paralysis of larynx is:
| A |
Puberuophonia |
|
| B |
Phonasthenia |
|
| C |
Dysphonia plicae ventricularis |
|
| D |
Normal or good voice |
Ans. is d i.e. normal or good voice
Management
- Lateralization of cord by arytenoidectomy, endoscopic surgery, thyroplasty type II, cordectomy
- In emergency cases -Tracheostomy may be required
Also know
- Generally patients with bilateral recurrent laryngeal nerve palsy have a recent history of thyroid surgery or rarely an advanced malignant thyroid tumor.
- Most common presentation-Development of stridor following URI
- Since the voice of the patient is normal\it is diagnosed very late.
Injury to superior laryngeal nerve causes:
| A |
Hoarseness |
|
| B |
Paralysis of vocal cords |
|
| C |
No effect |
|
| D |
Loss of timbre of voice |
Injury to superior laryngeal nerve causes:
| A |
Hoarseness |
|
| B |
Paralysis of vocal cords |
|
| C |
No effect |
|
| D |
Loss of timbre of voice |
Ans. is d e. Loss of timbre of voice
Paralysis of Superior Laryngeal Nerve -causes paralysis of cricothyroid muscle which is a tensor of vocal cord.
Clinical Features
- Voice is weak and pitch cannot be raised.
- U/L Anaesthesia of larynx above the level of vocal cords causing occasional aspiration.
Paralysis of recurrent laryngeal nerve true is:
| A |
Common in (Lt) side |
|
| B |
50% idiopathic |
|
| C |
Cord will be laterally |
|
| D |
Speech therapy given |
Paralysis of recurrent laryngeal nerve true is:
| A |
Common in (Lt) side |
|
| B |
50% idiopathic |
|
| C |
Cord will be laterally |
|
| D |
Speech therapy given |
Ans. is a i.e. Common in (left) side
Unilateral Recurrent Laryngeal Nerve Palsy
- More common on left side than right side because of the longer and more convoluted course of the left recurrent laryngeal nerve (Rt side is involved only in 3-30% cases) (i.e. option a is correct)
- Most unilateral vocal cord paralysis are secondary to surgery (i.e. option b is incorrect)
- Unilateral injury to recurrent laryngeal nerve leads to ipsilateral paralysis of all intrinsic muscles except cricothyroid (which is an adductor of vocal cord). The vocal cord thus assumes a median or paramedian position which does not move laterally on deep inspiration (i.e. option c is incorrect)
Clinical Features
- Asymptomatic in 1 /3rdcases
- In rest of the patients there may be some voice problem i.e. Dysphonia – the voice is hoarse & becomes weak with use. This gradually improves with time due to compensation by the healthy cord which crosses the midline to meet the paralysed one. Generally no speech therapy is required (i.e. option d is incorrect).
The voice is not affected in:
| A |
Unilateral abductor palsy |
|
| B |
Unilateral adductor palsy |
|
| C |
B/L superior laryngeal palsy |
|
| D |
Total adductor palsy |
The voice is not affected in:
| A |
Unilateral abductor palsy |
|
| B |
Unilateral adductor palsy |
|
| C |
B/L superior laryngeal palsy |
|
| D |
Total adductor palsy |
In U/L abductor palsy, the affected vocal cord assumes a median or paramedian position. The other is normal so one third patients are asymptomatic while others may have some voice change.
Cadaver like position of vocal cords is seen in
| A |
Both superior laryngeal nerve palsy |
|
| B |
Both recurrent laryngeal nerve palsy |
|
| C |
Both external laryngeal nerve palsy |
|
| D |
Both internal laryngeal nerve palsy |
Cadaver like position of vocal cords is seen in
| A |
Both superior laryngeal nerve palsy |
|
| B |
Both recurrent laryngeal nerve palsy |
|
| C |
Both external laryngeal nerve palsy |
|
| D |
Both internal laryngeal nerve palsy |
Recurrent Laryngeal Nerve paralysis:
If both recurrent laryngeal nerves are interrupted, the vocal cords lie in a cadaveric position in between abduction and adduction and phonation is completely lost.
When only one recurrent laryngeal nerve is affected, the opposite vocal cord compensates for it and phonation is possible but there is hoarseness of voice
Superior Laryngeal Nerve paralysis
It divides into external and internal laryngeal nerves. External laryngeal nerve supplies cricothyroid and inferior constrictor and internal laryngeal nerve supplies mucous membrane of the larynx upto the level of vocal folds:
- Asymmetric vocal cord tension
- Produces diplophonia
- Loss of vocal fold tension (lowers pitch of voice)
- Inaccurate vocal cord apposition
- Paralysed side slightly shortened and bowed
- May be depressed below level of normal side
- Rotation of AP axis of vocal cords
- Posterior commissure points to side of paralysis
- Loss of laryngeal sensation and increased risk of aspiration
