

Megaloblastic anemia
Megaloblastic anemia is due to –
| A |
Defect in DNA synthesis |
|
| B |
Defect in RNA synthesis |
|
| C |
Defect in protein synthesis |
|
| D |
All |
Megaloblastic anemia is due to –
| A |
Defect in DNA synthesis |
|
| B |
Defect in RNA synthesis |
|
| C |
Defect in protein synthesis |
|
| D |
All |
Ans. is ‘a’ i.e., Defect in DNA synthesis
Megaloblastic anemia
- Megaloblastic anemia is an anemia which results from inhibition of DNA synthesis during red blood cell production.
- It is characterized by many large immature and dysfunctional red blood cells (megaloblasts) in the bone marrow, and also by hypersegmented neutrophils.
Pathogenesis of megaloblastic anemia
o Vit B1, and folic acid are required for DNA synthesis.
o Any factor that results in deficiency of vit B1, or folic acid will lead to defective DNA synthesis.
- Inadequate DNA synthesis results in defective nuclear maturation.
- However, the synthesis of RNA and proteins is not altered, so cytoplasmic maturation proceeds in advance of nuclear maturation —> Nuclear/Cytoplasmic asynchrony that results in formation of megaloblasts. o DNA synthesis is impaired in all proliferating cells.
1. Cells of bone marrow —> Precursors of RBCs, WBCs, Platelets.
2. Mucosal lining of G1T.
Megaloblastic anemia is/are not caused by ‑
| A |
Vitamin B12 deficiency |
|
| B |
Folic acid deficiency |
|
| C |
Sodium valproate |
|
| D |
All |
Megaloblastic anemia is/are not caused by ‑
| A |
Vitamin B12 deficiency |
|
| B |
Folic acid deficiency |
|
| C |
Sodium valproate |
|
| D |
All |
Ans. is ‘c’ i.e., Sodium valproate
Vitamin B12 deficiency, folic acid deficiency and alcohol cause megaloblastic anemia.
o Amongst anticonvulsants, phenytoin and phenobarbitone cause megaloblastic anemia (not sodium valproate) o Aplastic anemia does not cause megaloblastic anemia.
All are true in megaloblastic anaemia except –
| A |
Microcytes |
|
| B |
Megakaryocytes |
|
| C |
Decrease in Platelets |
|
| D |
Neurological symptoms |
All are true in megaloblastic anaemia except –
| A |
Microcytes |
|
| B |
Megakaryocytes |
|
| C |
Decrease in Platelets |
|
| D |
Neurological symptoms |
Ans. is ‘a’ i.e., Microcytes


Megaloblastic anemia due to folic acid deficiency is commonly due to:
| A |
Inadequate dietary intake |
|
| B |
Defective intestinal absorption |
|
| C |
Absence of folic acid binding protein in serum |
|
| D |
Absence of glutamic acid in the intestine |
Megaloblastic anemia due to folic acid deficiency is commonly due to:
| A |
Inadequate dietary intake |
|
| B |
Defective intestinal absorption |
|
| C |
Absence of folic acid binding protein in serum |
|
| D |
Absence of glutamic acid in the intestine |
Answer is A (Inadequate dietary intake)
Folic acid deficiency most commonly results from either decreased dietary intake or increased metabolic demand. Amongst the options provided decreased dietary intake is the single best answer.
Megaloblastic anemia
1. Cobalamine deficiency
Most common cause is Malabsorption
‘The dietary intake qfcobalamine is more than adequate for body’s requirement except in complete vegetarians and their breast fed infants. Thus deficiency of cobaMmine is almost always due to malabsorption’
2. Folate deficiency
Most common cause is either decreased dietary intake or increased metabolic demand.
The dietary intake offolic acid is marginal in many parts of the world. Furthermore because the body’s stores of Folate are low, folic acid deficiency can arise rather suddenly during periods of decreased dietary intake or increased metabolic demand’
Which of the following is not a feature of megaloblastic anaemia:
September 2010
| A |
Thrombocytopenia |
|
| B |
Megakaryocytes |
|
| C |
Reticulocytosis |
|
| D |
Howell-jolley bodies |
Which of the following is not a feature of megaloblastic anaemia:
September 2010
| A |
Thrombocytopenia |
|
| B |
Megakaryocytes |
|
| C |
Reticulocytosis |
|
| D |
Howell-jolley bodies |
Ans. C: Reticulocytosis
The blood film suggestive of vitamin B12 deficiency includes:
- Decreased red blood cell (RBC) count and hemoglobin levels.
- Increased mean corpuscular volume (MCV, >95 fl) and mean corpuscular hemoglobin (MCH)
- Normal mean corpuscular hemoglobin concentration (MCHC, 32-36 g/dL)
- The reticulocyte count is decreased due to destruction of fragile and abnormal megaloblastic erythroid precursor.
- The platelet count may be reduced.
- Neutrophil granulocytes may show multisegmented nuclei (“senile neutrophil”).
- Anisocytosis (increased variation in RBC size) and poikilocytosis (abnormally shaped RBCs).
- Macrocytes (larger than normal RBCs) are present.
- Ovalocytes (oval-shaped RBCs) are present.
- Howell-Jolly bodies (chromosomal remnant) also present
Which of the following does not indicate megaloblastic anemia?
| A |
Increased reticulocyte count |
|
| B |
Raised Bilirubin |
|
| C |
Mild splenomegaly |
|
| D |
Nucleated RBC |
Which of the following does not indicate megaloblastic anemia?
| A |
Increased reticulocyte count |
|
| B |
Raised Bilirubin |
|
| C |
Mild splenomegaly |
|
| D |
Nucleated RBC |
Reticulocyte count is decreased due to destruction of fragile and abnormal megaloblastic erythroid precursors.
Megaloblastic anemia is characterized by hypercellular bone marrow with abnormally large nucleated RBC, raised unconjugated bilirubin and mild splenomegaly.
Erythroid activity in the marrow is enhanced, although the megaloblastic cells die before they are released, accounting for the reduced reticulocyte count.
Most characteristic of megaloblastic anemia ‑
| A |
Target cell |
|
| B |
Macrocyte |
|
| C |
Microovalocyte |
|
| D |
Macroovalocyte |
Most characteristic of megaloblastic anemia ‑
| A |
Target cell |
|
| B |
Macrocyte |
|
| C |
Microovalocyte |
|
| D |
Macroovalocyte |
Ans. is ‘d’ i.e., Macroovalocyte
Characteristic blood picture in megaloblastic anemia ‑
| A |
Macrocytosis and increased reticulocyte count |
|
| B |
Macrocytosis and decreased reticulocyte count |
|
| C |
Microcytosis and increased reticulocyte count |
|
| D |
Microcytosis and decreased reticulocyte count |
Characteristic blood picture in megaloblastic anemia ‑
| A |
Macrocytosis and increased reticulocyte count |
|
| B |
Macrocytosis and decreased reticulocyte count |
|
| C |
Microcytosis and increased reticulocyte count |
|
| D |
Microcytosis and decreased reticulocyte count |
Ans. is ‘b’ i.e., Macrocytosis and decreased reticulocyte count
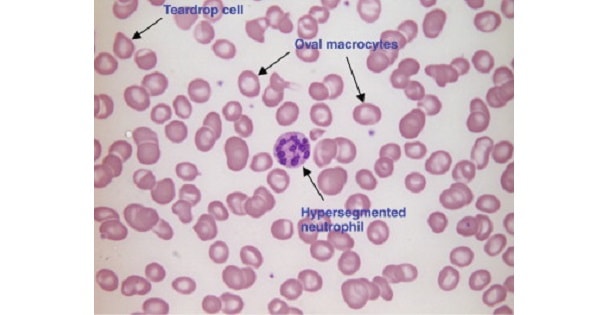
Findings of megaloblastic anemia
Peripheral blood
- Macrocytosis megaloblastic RBC → Due to nuclear/cytoplasmic asynchrony.
- Macrocytes lack central pallor of normal RBC.
- Anisopoikilocytosis → Marked variation in shape and size.
- Majority of RBCs appear as macroovalcytes.
- Few tear drop cells.
- Low reticulocyte count
- Some nucleated RBCs may appear (normally, during maturation of RBC, nucleus disappears).
- Hyper-segmented neutrophils → First manifestation of megaloblastic anemia.
- Large megakaryocytes with multilobate nuclei.
- Evidence of erythropoiesis : – Basophilic stippling, Cabott Ring, Howell-jolly bodies.
In the treatment of megaloblastic anemia, vitamin B12 and folic acid should be given together because
| A |
Vitamin B12 acts as a cofactor for digydrofolate reductase |
|
| B |
Folic acid alone causes improvement of anemic symptoms but neurological dysfunction continues |
|
| C |
Vitamin B12 deficiency may result in methylfolate trap |
|
| D |
Folic acid is required for conversion of methymalonyl-CoA to succinyl Co-A |
In the treatment of megaloblastic anemia, vitamin B12 and folic acid should be given together because
| A |
Vitamin B12 acts as a cofactor for digydrofolate reductase |
|
| B |
Folic acid alone causes improvement of anemic symptoms but neurological dysfunction continues |
|
| C |
Vitamin B12 deficiency may result in methylfolate trap |
|
| D |
Folic acid is required for conversion of methymalonyl-CoA to succinyl Co-A |
Ans. is ‘b’ i.e., Folic acid alone causes improvement of anemic symptoms but neurological dysfunction continues
Percentage absorption of iron falls progressively as iron deficiency is corrected.”
As the hemoglobin levels rise, erythropoietin stimulation decreases and the amount of iron reabsorbed is reduced”
Oral therapy for iron deficiency anemia
- A dose of 300 mg of elemental iron given per day in divided doses.
- 300 mg of elemental rion gives about 50 mg of absorbed iron per day (and not 100 mg of absorbed iron).
- Typically the Hb levels should be fully corrected within I month of initiating therapy in the absence of continuing blood loss (and not after six months).
- Treatment should not be stopped after normalizing of Hb, but continued for an additional 4 to 6 months to replenish body iron stores.
Which of the following does not indicate megaloblastic anemia
| A |
Increased reticulocyte count |
|
| B |
Raised Bilirubin |
|
| C |
Mild splenomegaly |
|
| D |
Nucleated RBC |
Which of the following does not indicate megaloblastic anemia
| A |
Increased reticulocyte count |
|
| B |
Raised Bilirubin |
|
| C |
Mild splenomegaly |
|
| D |
Nucleated RBC |
Ans. a. Increased reticulocyte count
- Megaloblastic anemia is characterized by hypercellular bone marrow with abnormally large nucleated RBC, raised unconjugated bilirubin and mild splenomegaly
Characteristic Features of Megaloblastic Anemia
- Bone marrow: Hypercellular with a decreased myeloid/erythroid ratio and abundant stainable iron
- RBC precursors: Abnormally large° and have nuclei that appear much less mature than would
- be expected from the development of the cytoplasm (nuclear-cytoplasmic asynchrony°).
- Nuclear chromatin is more dispersed than expected and it condenses in a peculiar fenestrated pattern°
- Raised unconjugated bilirubin°
- Mild reversible splenomegaly° (Wintrobes 12/e p1151)

