
PENICILLIN
| A | Inability of penicillin to penetrate the membrane of S. aureus | |
| B | Production of penicillinase by S. aureus | |
| C | Production of penicillin acetylase by S. aureus | |
| D | Lack of penicillin binding sites on S. aureus |
| A | Inability of penicillin to penetrate the membrane of S. aureus | |
| B | Production of penicillinase by S. aureus | |
| C | Production of penicillin acetylase by S. aureus | |
| D | Lack of penicillin binding sites on S. aureus |
Staphylococci are Gram-positive, non-sporeforming cocci. Clinically, their antibiotic resistance poses major problems. Many strains produce 13-lactamase (penicillinase), an enzyme that destroys penicillin by opening the lactam ring. Drug resistance, mediated by plasmids, may be transferred by transduction.
| A | Methicillin | |
| B | Carbenicillin | |
| C | Nafcillin | |
| D | Oxacillin |
| A | Methicillin | |
| B | Carbenicillin | |
| C | Nafcillin | |
| D | Oxacillin |
Carbenicillin
All of the following are therapeutic uses of penicillin G, EXCEPT:
| A |
Bacterial meningitis |
|
| B |
Rickettisial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
All of the following are therapeutic uses of penicillin G, EXCEPT:
| A |
Bacterial meningitis |
|
| B |
Rickettisial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
Majority of gram negative bacilli (except fewE.coli, Proteus), Mycobacterium tuberculosis, rickettsiae, chlamydiae, protozoa, fungi and viruses are totally insensitive to PnG (Benzyl Penicillin).
Ref: Essentials of Pharmacology By K D Tripathi, 5th Edition, Page 655; Drug Reference for Ems Providers By Richard K. Beck, 2001, Page 617.
Which one of the following drugs is an antipseudomonal penicillin?
| A |
Cephalexin |
|
| B |
Cjoxacillin |
|
| C |
Piperacillin |
|
| D |
Dicloxacillin |
Which one of the following drugs is an antipseudomonal penicillin?
| A |
Cephalexin |
|
| B |
Cjoxacillin |
|
| C |
Piperacillin |
|
| D |
Dicloxacillin |
Antipseudomonal penicillins include the carboxypenicillin and the ureidopenicillins.
Piperacillin belongs to the group of Ureidopenicillins. Antipseudomonal Penicillins Mezlocillin, piperacillin, and ticarcillin are parenteral antibiotics.
Ref: Essentials of Pharmacology By K D Tripathi, 5th Edition, Pages 660, 661, 658, 659; Drug Reference for Ems Providers By Richard K. Beck, 2001, Page 617.
All of the following statements about Penicillin Binding Proteins (PBPs) are true, EXCEPT:
| A |
PBP’s are essential for cell wall synthesis |
|
| B |
PBP’S are localized on the outer face of cell wall |
|
| C |
PBP’s act as carboxypeptidases and traspeptidases |
|
| D |
Alteration in PBP’s is the primary bases of resistance in MRSA |
All of the following statements about Penicillin Binding Proteins (PBPs) are true, EXCEPT:
| A |
PBP’s are essential for cell wall synthesis |
|
| B |
PBP’S are localized on the outer face of cell wall |
|
| C |
PBP’s act as carboxypeptidases and traspeptidases |
|
| D |
Alteration in PBP’s is the primary bases of resistance in MRSA |
All of the following statements about Penicillin Resistance is true, EXCEPT:
| A |
β- Lactamase production is the most common mechanism of resistance |
|
| B |
Alteration in target PBPs is an important resistance mechanism in Gram negative bacteria |
|
| C |
Alteration in permeability / penetration of antibiotic causes resistance only in Gram negative bacteria |
|
| D |
β-Lactamase production causes resistance in both Gram positive and Gram negative bacteria |
All of the following statements about Penicillin Resistance is true, EXCEPT:
| A |
β- Lactamase production is the most common mechanism of resistance |
|
| B |
Alteration in target PBPs is an important resistance mechanism in Gram negative bacteria |
|
| C |
Alteration in permeability / penetration of antibiotic causes resistance only in Gram negative bacteria |
|
| D |
β-Lactamase production causes resistance in both Gram positive and Gram negative bacteria |
Penicillin would be LEAST effective in treating:
| A |
Syphilis |
|
| B |
Streptococcal pharyngitis |
|
| C |
Pneumococcal pneumonia |
|
| D |
Mycoplasma pneumonia |
Penicillin would be LEAST effective in treating:
| A |
Syphilis |
|
| B |
Streptococcal pharyngitis |
|
| C |
Pneumococcal pneumonia |
|
| D |
Mycoplasma pneumonia |
Mycoplasma organisms do have a cell wall and are therefore resistant to penicillin.
Other forms of bacteria that lack a cell wall are spheroplasts and protoplasts, which are formed from gram-negative and gram-positive bacteria, respectively, through the action of penicillin or by other procedures that remove the cell wall or interfere with its formation.
The other organisms listed in the question are all susceptible to the action of penicillin.
Tetracyclines, erythromycin and the aminoglycosides are effective antibiotics for the treatment of mycoplasmal infections.
The molecular basis of penicillin resistance in S.Pneumoniae is:
| A |
Alteration of penicillin-binding protein |
|
| B |
Alteration in cell membranes |
|
| C |
Alteration in the cell wall |
|
| D |
None of the above |
The molecular basis of penicillin resistance in S.Pneumoniae is:
| A |
Alteration of penicillin-binding protein |
|
| B |
Alteration in cell membranes |
|
| C |
Alteration in the cell wall |
|
| D |
None of the above |
The molecular basis of penicillin resistance in S. pneumoniae is the alteration of penicillin-binding protein (PBP) genes which result in lower affinity for penicillins.
Penicillin G is the drug of choice for disease caused by susceptible organisms, including community-acquired pneumonia.
Ref: Harisson, Edition – 18, Page 1156
The drug of choice for the microorganism shown in the photograph is ? 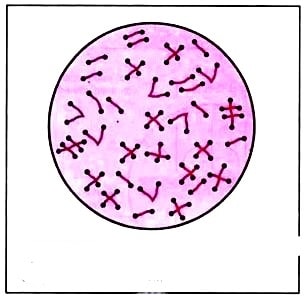
| A |
Tetrarycline. |
|
| B |
Vancomycin. |
|
| C |
Penicillin. |
|
| D |
Ampicillin. |
The drug of choice for the microorganism shown in the photograph is ?
| A |
Tetrarycline. |
|
| B |
Vancomycin. |
|
| C |
Penicillin. |
|
| D |
Ampicillin. |
Ans:C.)Penicillin.
The organism shown in the picture above represents Corynebacterium diphtheriae .
Corynebacterium diphtheriae
- Corynebacterium diphtheriae is the pathogenic bacterium that causes diphtheria. It is also known as the Klebs-Löffler bacillus.
- Corynebacterium diphtheriae is a nonmotile, noncapsulated, club-shaped, Gram-positive,pleomorphic bacillus.They have the characteristic of forming irregular, club-shaped or V-shaped arrangements in normal growth. They undergo snapping movements just after cell division, which brings them into characteristic forms resembling Chinese letters.Special stains like Alberts’s stain are used to demonstrate the metachromatic granules formed in the polar regions. The granules are called as polar granules, Babes Ernst granules.
- There are two types of clinical diphtheria: nasopharyngeal and cutaneous.
- Treatment:
- Antibiotics (e.g., penicillin and erythromycin) and passive immunization with diphtherial antitoxin.
Which of the following organisms, when isolated in the blood, requires the synergistic activity of penicillin plus an aminoglycoside for appropriate therapy-
| A |
Enterococcus faecalis |
|
| B |
Staphylococcus aureus |
|
| C |
Str. pneumoniae |
|
| D |
Bacteroides fragilis |
Which of the following organisms, when isolated in the blood, requires the synergistic activity of penicillin plus an aminoglycoside for appropriate therapy-
| A |
Enterococcus faecalis |
|
| B |
Staphylococcus aureus |
|
| C |
Str. pneumoniae |
|
| D |
Bacteroides fragilis |
Ans. is ‘a’ i.e., Enterococcus faecalis
“Unlike streptococci, enterococci are not reliably killed by penicillin or ampicillin alone. Because of synergistic action of Penicillin and aminoglycoside against enterococci combination therapy is recommended “.
Plant penicillin is
| A |
Carbamate |
|
| B |
OPC |
|
| C |
Endrin |
|
| D |
DDT |
Plant penicillin is
| A |
Carbamate |
|
| B |
OPC |
|
| C |
Endrin |
|
| D |
DDT |
C i.e. Endrin
Drug that inhibits cell wall synthesis is?
| A |
Tetracyc I ins |
|
| B |
Penicillins |
|
| C |
Aminoglycosides |
|
| D |
Chloramphenicol |
Drug that inhibits cell wall synthesis is?
| A |
Tetracyc I ins |
|
| B |
Penicillins |
|
| C |
Aminoglycosides |
|
| D |
Chloramphenicol |
Ans. is ‘b’ i.e., Penicillins
One of the following is not penicillinase susceptible‑
| A |
Amoxicillin |
|
| B |
Penicillin G |
|
| C |
Piperacillin |
|
| D |
Cloxacillin |
One of the following is not penicillinase susceptible‑
| A |
Amoxicillin |
|
| B |
Penicillin G |
|
| C |
Piperacillin |
|
| D |
Cloxacillin |
Ans. is ‘d’ i.e., Cloxacillin
Penicillinase – resistant penicillins – Methicillin, Cloxacillin, Oxacillin, flucloxacillin, dicloxacillin, Nafcillin.
Acid Labile penicillin is-
| A |
Cloxacillin |
|
| B |
Flucloxacillin |
|
| C |
Methicillin |
|
| D |
Phenoxy Methyl penicillin |
Acid Labile penicillin is-
| A |
Cloxacillin |
|
| B |
Flucloxacillin |
|
| C |
Methicillin |
|
| D |
Phenoxy Methyl penicillin |
Ans. is ‘c’ i.e., Methicillin
o Gastric acid destroyes the penicillins and decreases their bioavailibility.
o All penicillins are acid labile accept phenoxymethyl penicillin (penicillin V), Cloxacillin, Flucloxacillin, Oxacillin, Dicloxacillin, ampicillin.
Note – Cloxacillin, flucloxacillin, oxacillin, and dicloxacillin are resistant to both acid as well as penicillinase.
Which among the following is not a beta lactamase resistant Penicillin?
| A |
Methicillin |
|
| B |
Carbenicillin |
|
| C |
Nafcillin |
|
| D |
Oxacillin |
Which among the following is not a beta lactamase resistant Penicillin?
| A |
Methicillin |
|
| B |
Carbenicillin |
|
| C |
Nafcillin |
|
| D |
Oxacillin |
Ans. is ‘b’ i.e., Carbenicillin
Penicillinase resistant penicillin is-
| A |
Methicillin |
|
| B |
Ampicillin |
|
| C |
Carbenicillin |
|
| D |
Ticarcillin |
Penicillinase resistant penicillin is-
| A |
Methicillin |
|
| B |
Ampicillin |
|
| C |
Carbenicillin |
|
| D |
Ticarcillin |
Ans. is ‘a’ i.e., Methicillin
All of the following statements about Penicillin resistance are true, Except –
| A |
beta-Lactamase production is the most common mechanism of resistance |
|
| B |
Alteration in target PBPs is an important resistance mechanism in gram negative bacteria |
|
| C |
Alteration in permeability/penetration of antibiotic causes resistance only in gram negative bacteria |
|
| D |
beta-Lactamase production causes resistance in both gram positive and gram negative bacteria |
All of the following statements about Penicillin resistance are true, Except –
| A |
beta-Lactamase production is the most common mechanism of resistance |
|
| B |
Alteration in target PBPs is an important resistance mechanism in gram negative bacteria |
|
| C |
Alteration in permeability/penetration of antibiotic causes resistance only in gram negative bacteria |
|
| D |
beta-Lactamase production causes resistance in both gram positive and gram negative bacteria |
Ans. is b i.e., Alteration in target PBPs is an important resistance mechanism in gram negative bacteria
PENICILLIN RESISTANCE
o Mechanism of resistance are ‑
Penetration into the cell
o Gram negative bacteria have an outer membrane just outside the cell wall.
o Outer membrane is not present in gram positive bacteria, so this mechanism of resistance is not for gram positive organisms.
beta-lactamase (Penicillinase) Production
o This is the most common mechanism
o Both gram positive and gram negative organism produce beta-lactamase which open the beta-lactam ring and inactivate the antibiotic.
Altered penicillin bindinE protein (PBP)
o Bacteria can alter the structure of penicillin binding protein, which is not other than transpeptidase.
o So, penicillin can not bind to the site where it acts.
o MRSA defends itself in this way.
o Organism resistant to methicillin, MRSA is resistant to all other beta-lactam antibiotics.
All of the following are therapeutic uses of penicillin G, except –
| A |
Bacterial meningitis |
|
| B |
Rickettsial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
All of the following are therapeutic uses of penicillin G, except –
| A |
Bacterial meningitis |
|
| B |
Rickettsial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
Ans. is ‘b’ i.e., Rickettsial infection
Antibacterial spectrum of Penicillin G (Benzyl Penicillin)
o PnG is a narrow spectrum antibiotic
o Activity is limited primary to gram positive bacteria (and few others).
o Amongst gram negative organisms, penicillin has activity against gonococci, meningococci, few Ecoli & proteus. o Majority of gram negative bacilli are insensitive.
o M. Tuberculosis, Ricketsiae, chlamydia, protozoa, fungi and viruses are totally insensitive to penicillin G.
Penicillin G is the DOC for (Laurence 9th/e 218. Katzun_g 7301
|
1. |
Meningococcal meningitis |
7. |
Leptospira |
|
2. |
Bacillus anthracis (anthrax) |
8. |
Actinomyces israelii (Actinomycosis) |
|
3. |
Clostridium perfringens (gas gangrene) |
9. |
Borrelia burgdorferi (Lyme disease) |
|
4. |
Clostridium tetani (tetanus) |
10. |
Enterococci |
|
5. |
Corynebacterium diphtheriae |
11. |
Streptococci |
|
6. |
Treponema pallidum (syphilis) |
12. |
Susceptible pneumococci |
Dosage of benzyl penicillin in treatment of primary syphiis is –
| A |
1.2 MU single i.m. |
|
| B |
1.2 MU single i.v. |
|
| C |
2.4 MU single i.m. |
|
| D |
4.8 MU single i.m. |
Dosage of benzyl penicillin in treatment of primary syphiis is –
| A |
1.2 MU single i.m. |
|
| B |
1.2 MU single i.v. |
|
| C |
2.4 MU single i.m. |
|
| D |
4.8 MU single i.m. |
Ans. is ‘c’ i.e., 2.4 MU single i.m.
All of the following statement about penicillin G are true except –
| A |
It is actively secreted in tubules |
|
| B |
It is never administered orally |
|
| C |
It is effective against gram positive as well as gram negative bacteria |
|
| D |
It acts by inhibiting cell wall synthesis |
All of the following statement about penicillin G are true except –
| A |
It is actively secreted in tubules |
|
| B |
It is never administered orally |
|
| C |
It is effective against gram positive as well as gram negative bacteria |
|
| D |
It acts by inhibiting cell wall synthesis |
Ans. is ‘b’ i.e., It is never administered orally
o Here comes the confusing one.
o In this question there is confusion between option ‘b’ and ‘c’.
o First see option ‘b’
Penicillin G is degraded by acid.
So, most of the time it is given by injection.
But oral preparations are also available “Despite the convenience of oral administration of penicillin G, this route should be used only in infections in which clinical experience has proven its efficacy”. -Goodman & Gilman
So, option b is absolutely wrong and is the answer of our question.
o Now see option C
Penicillin G is a narrow spectrum penicillin, i.e. activity is limited primarily to gram positive bacteria but it has activity against some gram negative organisms also, e.g. meningococci, gonococci (if strains are sensitive), few strains of E.coli.
So, option C is partially correct.
About other options
o Penicillin is primarily excreted by kidney –> 10-20% by glomerular filtration and 80-90% by active tubular secretion —> Active secretion‘is inhibited by probenacid which increases blood concentration of penicillin. o Penicillin acts by inhibiting cell wall synthesis.
Also know
o Penicillin G (benzyl penicillin) has a short VA. So, it has to be given 6-12 hourly.
o Procaine penicillin and benzathine penicillin (longest acting) are long acting due to slow release.
o Extended (broad) spectrum penicillins (Aminopenicillins, Carboxypenicillins and ureidopenicillins) are active against gram negative organisms as well (in addition to gram positive oraganisms, though their activity against gram positive organisms is less than penicillin G).
o Activity of penicillins against gram positive organisms —> Penicillin G (max) > Extendend spectrum penicilins > b- lactamase resistant penicillins (methicillin & others).
When allergic to penicillin, other drugs contraindicated –
| A |
Monobactams |
|
| B |
Carbapenems |
|
| C |
Cephalosporins |
|
| D |
b and c |
When allergic to penicillin, other drugs contraindicated –
| A |
Monobactams |
|
| B |
Carbapenems |
|
| C |
Cephalosporins |
|
| D |
b and c |
Ans. is ‘b’ i.e., Carbapenems; ‘c’ i.e., Cephalosporins
Allergic reaction to penicillin
o The main hazard with the penicillin is allergic reactions.
o These include itching, rashes (eczematous or urticaria), fever and angioedema.
o Anaphylactic shock can occur though rarely (1 in 10,000).
o Allergies are least when penicillins are given orally and most likely with local application.
o Penicillin G is the most common drug implicated in drug allergy —› Procaine penicillin preparation of PnG has the highest incidence (procaine is itself allergic).
o There is cross-allergy between all the various forms of penicillin, probably due to in part to their common structure, and in part to the degradation products common to them all.
o There is partial cross-allergy between penicillins and cephalosporins (5-10%).
Carbapenems also have some cross-allergy with penicillins, but less than cephalosporins.
o Monobactoms (aztreonam) do not have cross reactivity.
o So, Pt with penicillin ‘G’ allergy should not receive any penicillin, cephalosporins and carbapenems (Imipenem. meropenem). Monobactams (Aztreonam) are safe
“Order of cross reactivity with penicillin G :- Other penicillins (maximum) > Cephalosporins > Carbapenems
> Monobactams (no cross reactivity)”.
All of the following statements about penicillin binding proteins (PBP) are true, except –
| A |
PBP’S are localized on the outer face of cell wall |
|
| B |
PBP’s are essential for cell wall synthesis |
|
| C |
PBP’s act as carboxypeptidases and traspeptidases |
|
| D |
Alteration in PBP’s is the primary bases of resistance in MRSA |
All of the following statements about penicillin binding proteins (PBP) are true, except –
| A |
PBP’S are localized on the outer face of cell wall |
|
| B |
PBP’s are essential for cell wall synthesis |
|
| C |
PBP’s act as carboxypeptidases and traspeptidases |
|
| D |
Alteration in PBP’s is the primary bases of resistance in MRSA |
Ans. is ‘a’ i.e., PBP’S are localized on the outer face of cell wall
Penicillin binding proteins (PBPs)
o S. aureus strains have four normal penicillin binding proteins (PBPs) anchored on the cytoplasmic membrane.
o PBPs are essential for cell wall synthesis by participating in the crosslinking of the peptidoglycan of bacterial cell wall.
o PBPs act as transpeptidases and carboxypeptidases.
o These PBPs have activity similar to that serine protease and high affinity for beta-lactam agent.
o When bea-lactam antibiotic binds to PBPs, the PBPs are not available to function in the assembly of cell wall causing bacterial death.
o PBP2a on the other hand, is not part of the intrinsic set of PBPs of s.aureus but is an inducible acquired protein (extra PBP) that is produced only by methicillin resistant s.aureus (MRSA).
o PBP2a has very low affinity for beta-lactam antibiotic —> beta-lactam antibiotics cannot bind to its receptor (PBP) and the organism (MRSA) is resistant to all available beta-lactam antibiotics.
o PBP2a is encoded by the mec A gene, which is not present in methicillin susceptible s.aureus (Present only in MRSA).
Treatment for clostridial myonecrosis is?
| A |
Amikacin |
|
| B |
Penicillin |
|
| C |
Ampicillin |
|
| D |
Gentamycin |
Treatment for clostridial myonecrosis is?
| A |
Amikacin |
|
| B |
Penicillin |
|
| C |
Ampicillin |
|
| D |
Gentamycin |
Ans. is ‘b’ i.e., Penicillin
o Antibiotic of choice for clostridia! myonecrosis (gas gangrene) is penicillin.
Drug of choice for Treponema Pallidum iS?
| A |
Penicillin G |
|
| B |
Tetracycline |
|
| C |
Azithromycin |
|
| D |
Doxycycline |
Drug of choice for Treponema Pallidum iS?
| A |
Penicillin G |
|
| B |
Tetracycline |
|
| C |
Azithromycin |
|
| D |
Doxycycline |
Ans. is ‘a’ i.e., Penicillin G
The drug of choice for thoracic actinomycosis is-
| A |
Amphotericin – B |
|
| B |
Penicillin |
|
| C |
Cotrimoxazole |
|
| D |
Itraconazole |
The drug of choice for thoracic actinomycosis is-
| A |
Amphotericin – B |
|
| B |
Penicillin |
|
| C |
Cotrimoxazole |
|
| D |
Itraconazole |
Ans. is ‘b’ i.e., Penicillin
Penicillin is the drug of choice for all types of actinomycosis.
Which of the following is not an ototoxic drug ‑
| A |
Neosporin |
|
| B |
Penicillin G |
|
| C |
Kanamycin |
|
| D |
Cisplatin |
Which of the following is not an ototoxic drug ‑
| A |
Neosporin |
|
| B |
Penicillin G |
|
| C |
Kanamycin |
|
| D |
Cisplatin |
Ans. is ‘b’ i.e., Penicillin G
Important ototoxic drugs
o Aminoglycosides
o Cisplatin
o Furosemide
o Deferoxamine
o Quinine
o Chloroquine
o Interferons
o Erythromycin
o Bleomycin
o Aspirin
One of the following in high doses can cause convulsions ‑
| A |
Penicillin |
|
| B |
Aminoglycosides |
|
| C |
Erythromycin |
|
| D |
All |
One of the following in high doses can cause convulsions ‑
| A |
Penicillin |
|
| B |
Aminoglycosides |
|
| C |
Erythromycin |
|
| D |
All |
Ans. is ‘a’ i.e., Penicillin
Drugs causing seizures
o Lactam antibiotics
o Local anaesthetics
o Quinolones
o Cyclosporine
o Acyclovir & Ganciclovir
o OKT3
o Isoniazid
o Tacrolimus
o Meperidine
o Interferons
o Tramadol
o Antidepressants
o Antipsychotics
o Lithium
o Theophylline
o Alcohol withdrawl
o Barbiturate withdrawl
o Benzodiazepine withdrawl
A child presented with fever for 2 days, altered sensorium and purpuric rashes. His blood pressure is 90/60 mmHg. Treatment of choice is –
| A |
IV Quinine |
|
| B |
IV Artesunate |
|
| C |
IV Penicillin |
|
| D |
Chloroquine |
A child presented with fever for 2 days, altered sensorium and purpuric rashes. His blood pressure is 90/60 mmHg. Treatment of choice is –
| A |
IV Quinine |
|
| B |
IV Artesunate |
|
| C |
IV Penicillin |
|
| D |
Chloroquine |
Ans. is ‘c’ i.e., Penicillin
o The clinical presentation of fever, altered sensorium and purpuric rashes, is highly suggestive of meningiococcal meningitis.
o Purpuric rash in quite characteristic of meningococcemia.
o I.V. Penicillin is the treatment of choice for meningioccal inf. among the given options.
o The DOC for meningiococcal infection is
o 111rd generation cephalosporin e.g. Cefotoxime, Ceftriaxone.
TOC for penicillin resistant gonorrhoea
| A |
Ciprofloxacin |
|
| B |
Ceftriaxone |
|
| C |
Streptomycine |
|
| D |
Erythromycin |
TOC for penicillin resistant gonorrhoea
| A |
Ciprofloxacin |
|
| B |
Ceftriaxone |
|
| C |
Streptomycine |
|
| D |
Erythromycin |
B i.e. Ceftriaxone
Neisseria gonorrhea is a gram negative, aerobic, non-motile, non-sporeforming, diplo/mono-cocciQ, exclusively a human pathogen that principally infects host columnar epithelium. It is oxidase positive like other Neisseria species, from which it is distinguished by their ability to grow on selective media & to utilize glucose but not maltose, sucrose or lactose.
Gonorrhoea is, the second most common (after Chlamydia trachomatis which is the most common) genital /sexually transmitted infection in US, UK and other developed countriesQ (Harrison 1442; Rook’s 34.24). The incidence of gonorrhea is higher in developing countriesQ than industrialized nations predominantly affecting young, nonwhite, unmarried, less educated urban population. (Harrison 1220)
Chlamydia trachomatis is the most common cause of non gonococcal urethritis (NGU) and postgonococcal urethritis (PGU)Q. PGU refers to NGU developing in men 2-3 weeks after treatment of gonococcal urethritis with single doses of agents such as penicillin or cephalosporins which lack activity against Chlamydia. In US most of acute urethritis cases are NGU and C. trachomatis is implicated in most (30-50%) of these casesQ. The other causes of NGU are Ureaplasma urealyticum, Mycoplasma genitalium, Trichomonas vaginalis and herpes simplex virus (HSV).
Gonorrhoea is a STD which commonly manifests as cervicitis (primary site of infection in females), urethritis (most common/primary site of infection in males presenting as rapid onset severe burning dysuria with profuse purulent discharge)Q, proctitis & conjunctivitis. If untreated it can 1/t local complications such as endometritis, salpingitis, tuboovarian abscessQ, bartholinitis, peritonitis and perihepatitis (Fitz-Hugh Curtis Syndrome) in females; peri urethritis and epididymitisQ in male patients and ophthalmia neonatorum in new borns. Disseminated gonococcemia is uncommon & 1/t skin lesions, tenosynovitis, arthritis and in rare cases endocarditis & meningitis.
Because of ascending spread of infection testis is spared or (uncommonly) last to be involvedQ only after urethritis, prostatitis, epididymitis in gonorrhea.
Single dose regimens of 3rd generation cephalosporins ceftriaxone (IM) and cefixime (oral) are the mainstays of therapyQ for uncomplicated gonococcal infection of urethra, cervix, rectum, or pharynx. Septinomycin is an alternative (2nd) regimen for uncomplicated gonococcal infections in penicillin allergic patients. All 3 drugs are suitable for pregnant & breast feeding women.
The new management for complaints of urethral discharge involves a combined modality of treatment for N. gonorrhea and C. trachomatisQ as most cases are d/t coinfection with both pathogens and incorporate an agent eg. azithromycin or doxycycline that is effective agenist chlamydial infection. Pregnant women who should not take doxycycline, should receive concurrent treatment with a macrolide antibiotic for possible chlamydial infection.
|
Feature |
Gonococcus |
Syphilis |
|
Infect/ |
EpididymisQ |
TestisQ |
|
Involve |
|
|
|
Resistant structure (not involve) |
TestisQ |
EpididymisQ |
|
Infection |
Urethrae |
Blood |
|
spread |
(i.e. |
(i.e. testis is |
|
through |
Epididymis is |
involved & |
|
|
involved & |
epididymis is |
|
|
testis is spared) |
spared) |
DOC in primary syphillis is
| A |
Corticosteroid |
|
| B |
Oral Penicilline |
|
| C |
Benzathine Penicilline |
|
| D |
Crystalline Penicilline |
DOC in primary syphillis is
| A |
Corticosteroid |
|
| B |
Oral Penicilline |
|
| C |
Benzathine Penicilline |
|
| D |
Crystalline Penicilline |
C i.e. Benzathine penicillin
Drug of choice for syphilis in a pregnant women
| A |
Azithromycin |
|
| B |
Penicillin |
|
| C |
Tetracycline |
|
| D |
Ceftriaxone |
Drug of choice for syphilis in a pregnant women
| A |
Azithromycin |
|
| B |
Penicillin |
|
| C |
Tetracycline |
|
| D |
Ceftriaxone |
B i.e. Penicillin
Penicillin is the only recommended agent for treatment of syphilis in pregnancyQ. If the patient has a documented penicillin allergy, desensitization and penicillin therapy should be given.
A sewage worker presents to the Emergency department with fever and jaundice. Laboratory findings reveal an elevated BUN and serum creatinine suggestive of renal failure. Which of the following antiboitics is recommended?
| A |
Cotrimaxozole |
|
| B |
Erythromycin |
|
| C |
Ciprofloxacin |
|
| D |
Penicillin G |
A sewage worker presents to the Emergency department with fever and jaundice. Laboratory findings reveal an elevated BUN and serum creatinine suggestive of renal failure. Which of the following antiboitics is recommended?
| A |
Cotrimaxozole |
|
| B |
Erythromycin |
|
| C |
Ciprofloxacin |
|
| D |
Penicillin G |
Ans. is ‘d’ i.e. Penicillin G
o Presence of fever, jaundice and renal failure in a sewage worker (contact with rat urine) suggests a diagnosis of Wen syndrome or Icterohemorrhageic fever caused by leptospirae.
o Penicillin G (intravenously) is the recommended agent.
“In severe illness, I.V benzyl penicillin is the drug of choice, for milder infections a 7-10 days course of oral amoxicillin appropriate.” – Green wood I 6th/e 355
o Patients allergic to penicillin can be treated with erythromycin.
Treatment of spreading streptococcal cellulitis is‑
| A |
Erythromycin |
|
| B |
Penicillin |
|
| C |
Tetracycline |
|
| D |
Chloramphenicol |
Treatment of spreading streptococcal cellulitis is‑
| A |
Erythromycin |
|
| B |
Penicillin |
|
| C |
Tetracycline |
|
| D |
Chloramphenicol |
Ans. is ‘b’ i.e., Pencillin
Treatment of contaminated wound in Gas Gangrene is
| A |
Debridement of wound |
|
| B |
Systemic penicillin |
|
| C |
Metronidazole Administration |
|
| D |
a and b |
Treatment of contaminated wound in Gas Gangrene is
| A |
Debridement of wound |
|
| B |
Systemic penicillin |
|
| C |
Metronidazole Administration |
|
| D |
a and b |
Ans. is ‘a’ i.e. Debridement of wound & ‘b’ i.e. Systemic penicillin
An old diabetic male presented with rapidly spreading infection of the external auditory canal with involvement of the bone and presence of granulation tissue. The drug of choice for this condition is:
| A |
Ciprofloxacin |
|
| B |
Penicillin |
|
| C |
Second generation cephalosporin |
|
| D |
Aminoglycosides |
An old diabetic male presented with rapidly spreading infection of the external auditory canal with involvement of the bone and presence of granulation tissue. The drug of choice for this condition is:
| A |
Ciprofloxacin |
|
| B |
Penicillin |
|
| C |
Second generation cephalosporin |
|
| D |
Aminoglycosides |
Rapidly spreading infection of external auditory canal, seen in diabetic patient with involvement of bone and presence of granulation tissue point towards malignant otitis externa as the diagnosis.
Treatment
- Includes correction of immunosuppression (when possible), local treatment of the auditory canal, long-term systemic antibiotic therapy, and in selected patients, surgery:
- In all cases, the external ear canal is cleansed and a biopsy specimen of the granulation tissue sent for culture.
- IV antibiotics is directed against the offending organism.
- For Pseudomonas aeruginosa, the most common pathogen, the regimen involves an antipseudomonal penicillin or cephalosporin (3rd generation piperacillin or ceftazidime) with an aminoglycoside. A fluoroquinolone antibiotic can be used in place of the aminoglycoside.
- Ear drops containing antipseudomonal antibotic e.g. ciproflaxacin plus a glucocorticoid is also used.
- Extensive surgical debridement once an important part of the treatment is now rarely needed.
A 3 year old child presents with fever and ear ache. On examination there is congested tympanic membrane with slight bulge. The treatment of choice is:
| A |
Myringotomy with penicillin |
|
| B |
Myringotomy with grommet |
|
| C |
Only antibiotics |
|
| D |
Wait and watch |
A 3 year old child presents with fever and ear ache. On examination there is congested tympanic membrane with slight bulge. The treatment of choice is:
| A |
Myringotomy with penicillin |
|
| B |
Myringotomy with grommet |
|
| C |
Only antibiotics |
|
| D |
Wait and watch |
Fever + earache + congested and bulging tympanic membrane in a four year old child points towards Acute suppurative otitis media as the diagnosis.
Antibiotics (Penicillin) form the mainstay of treatment of acute otitis media and should be administered in a child with Acute otitis media and once tympanic membrane is bulging, myringotomy should be done.
Grommet insertion is not indicated in Acute suppurative otitis media. It may be used in cases of myringotomy for serous or secretory otitis media.
True about quinsy is:
| A |
Penicillin is used in treatment |
|
| B |
Abscess is located in capsule |
|
| C |
Commonly occurs bilaterally |
|
| D |
Immediate tonsillectomy should be done |
True about quinsy is:
| A |
Penicillin is used in treatment |
|
| B |
Abscess is located in capsule |
|
| C |
Commonly occurs bilaterally |
|
| D |
Immediate tonsillectomy should be done |
- Quinsy is collection of pus outside the capsule (not in capsule) in peritonsillar area
- It is usually unilateral
- Patient presents with toxic symptoms due to septicemia as well as local symptoms (e.g. dribbling of saliva from mouth)
- Antibiotics: High-dose penicillin. (IV benzipenicillin) is the DOC. In patients allergic to penicillin, erythromycin is the DOC. If antibiotics fail to relieve the condition within 48 hours, then the abscess must be opened and drained.
Dosage and drug of choice for primary syphilis:
September 2012
| A |
Amoxicillin (500 mg for 5 days) |
|
| B |
Benzathine penicillin (2.4 mega units deep IM) |
|
| C |
Erythromycin (2 gm daily for 2 weeks) |
|
| D |
Doxycycline (100 mg daily for 2 weeks) |
Dosage and drug of choice for primary syphilis:
September 2012
| A |
Amoxicillin (500 mg for 5 days) |
|
| B |
Benzathine penicillin (2.4 mega units deep IM) |
|
| C |
Erythromycin (2 gm daily for 2 weeks) |
|
| D |
Doxycycline (100 mg daily for 2 weeks) |
Ans. B i.e. Benzathine penicillin (2.4 mega units deep IM)
Treatment of syphilis
- Primary or secondary syphilis – Benzathine penicillin G 2.4 million units intramuscularly (IM) in a single dose
- Early latent syphilis – Benzathine penicillin G 2.4 million units IM in a single dose
- Late latent syphilis or latent syphilis of unknown duration – Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals
- Pregnancy – Treatment appropriate to the stage of syphilis is recommended.
- In patients with a history of penicillin allergy, skin testing is recommended.
Which of the following is an anti-pseudomonal drug of penicillin class:
March 2013
| A |
Nafcillin |
|
| B |
Dicloxacillin |
|
| C |
Piperacillin |
|
| D |
Cloxacillin |
Which of the following is an anti-pseudomonal drug of penicillin class:
March 2013
| A |
Nafcillin |
|
| B |
Dicloxacillin |
|
| C |
Piperacillin |
|
| D |
Cloxacillin |
Ans. C i.e. Piperacillin
Extended-spectrum penicillin
- It is a group of antibiotics that has the widest antibacterial spectrum of all penicillins.
- It is also called antipseudomonal penicillins.
- This group includes the Aminopenicillins:
- Amoxicillin
- Ampicillin
- Epicillin
– Carboxypenicillins:
- Ticarcillin
- Carbenicillin Ureidopinicillin
- Azlocillin
- Mezlocillin
- Piperacillin
– Mecillinam
Dose and duration of benzathine penicillin for prophylaxis of rheumatic fever is:
September 2009
| A |
1.2 MU every 2 weeks |
|
| B |
1.2 MU every 4 weeks |
|
| C |
2.4 MU every 2 weeks |
|
| D |
2.4 MU every 4 weeks |
Dose and duration of benzathine penicillin for prophylaxis of rheumatic fever is:
September 2009
| A |
1.2 MU every 2 weeks |
|
| B |
1.2 MU every 4 weeks |
|
| C |
2.4 MU every 2 weeks |
|
| D |
2.4 MU every 4 weeks |
Ans. B: 1.2 MU every 4 weeks
Benzathine penicillin G 0.6-2.4 MU intramuscularly is given every 2-4 weeks as aqueous suspension.It releases penicillin extremely slowly-plasma concentrations are very low but remain effective for prophylactic purposes for up to one week. Low concentrations of penicillin prevent colonization by streptococci responsible for rheumatic fever. Benzathine
penicillin is given 1.2 MU every 4 weeks till 18 years of age or 5 years after an attack, whichever is more. Adverse drug reactions
- Hypersensitivity reaction without anaphylaxis.The most common reaction is idiopathic with a maculopapular or morbilliform rash. Anaphylaxis is rare (1-4 per 10,000 patients) but may be fatal.
- GI intolerance (with oral administration)
- Phlebitis at infusion sites and sterile abscesses at IM sites
- Jarisch-Herxheimer reaction (with treatment of syphilis or other spirochetal infections)
All of the following are true regarding penicillin except:
March 2005
| A |
Probenecid decreases it duration of action |
|
| B |
All penicillin are active against gram positive organisms |
|
| C |
Splits into 6-amino penicillanic acid by amidase |
|
| D |
Acts by inhibiting cell wall synthesis |
All of the following are true regarding penicillin except:
March 2005
| A |
Probenecid decreases it duration of action |
|
| B |
All penicillin are active against gram positive organisms |
|
| C |
Splits into 6-amino penicillanic acid by amidase |
|
| D |
Acts by inhibiting cell wall synthesis |
Ans. A: Probenecid decreases it duration of action
Drug interactions have been deliberately used to prolong the effect of penicillin, such as co-administering probenecid with penicillin prior to mass production of penicillin.
Because penicillin was difficult to manufacture, it was worthwhile to find a way to reduce the amount required. Probenecid retards the excretion of penicillin, so a dose of penicillin persists longer when taken with it and it allowed patients to take less penicillin over a course of therapy.
Drug used for prophylaxis of rheumatic heart disease:
March 2011
| A |
Sulfadiazine |
|
| B |
Phenoxy-methyl penicillin |
|
| C |
Benzathine penicillin |
|
| D |
All of the above |
Drug used for prophylaxis of rheumatic heart disease:
March 2011
| A |
Sulfadiazine |
|
| B |
Phenoxy-methyl penicillin |
|
| C |
Benzathine penicillin |
|
| D |
All of the above |
Ans. D: All of the above
Patients with acute rheumatic fever are susceptible to further attacks of the rheumatic fever if another streptococcal infection occurs, and a long term prophylaxis with penicillin should be given as benzathine penicillin 1.2 million U I/ M monthly or oral phenoxymethylpenicillin 250 mg 12 hourly
Sulfadiazine or erythromycin may be used if patient is allergic to penicillin
Treatment agent for scarlet fever is
| A |
Penicillin |
|
| B |
Ciprofloxacin |
|
| C |
Erythromycin |
|
| D |
Chloramphenicol |
Treatment agent for scarlet fever is
| A |
Penicillin |
|
| B |
Ciprofloxacin |
|
| C |
Erythromycin |
|
| D |
Chloramphenicol |
Ans. is ‘a’ i.e., Penicillin
Scarlet Fever
- Scarlet fever consists of streptococcal infection, usually pharyngitis, accompanied by a characteristic rash. The rash arises from the effects of one of three toxins, currently designated streptococcal pyrogenic exotoxins A, B, and C and previously known as erythrogenic or scarlet fever toxins.
- The symptoms of scarlet fever are the same as those of pharyngitis alone. The rash typically begins on the first or second day of illness over the upper trunk, spreading to involve the extremities but sparing the palms and soles.
- The rash is made up of minute papules, giving a characteristic “sandpaper” feel to the skin. Associated findings include circumoral pallor, “strawberry tongue” (enlarged papillae on a coated tongue, which later may become denuded), and accentuation of the rash in skinfolds (Pastia’s lines).
- Subsidence of the rash in 6-9 days is followed after several days by desquamation of the palms and soles
- Susceptibility to scarlet fever was correlated with results of the Dick test.
Treatment :
- Immediate hospitalization and isolation of the patient is indicated. Penicillin is the treatment of choice.
Carboxypenicillins true is all except ‑
| A |
Nephrotoxic |
|
| B |
Sensitive to penicillinase |
|
| C |
Effective against pseudomonas |
|
| D |
Platelet aggregation affected |
Carboxypenicillins true is all except ‑
| A |
Nephrotoxic |
|
| B |
Sensitive to penicillinase |
|
| C |
Effective against pseudomonas |
|
| D |
Platelet aggregation affected |
Ans. is ‘a’ i.e., Nephrotoxic
Carboxvpenicillins – Carbenicillin:
- It is active against pseudomonas and indole positive proteus.
- Klebsiella and gram positive cocci are unaffected by it
- It is neither penicillinase resistant nor acid resistant.
- It is inactive orally and is rapily excreted in urine in 1 hr.
- At high doses it can cause bleeding by interfering with platelet function due to perturbation of agonists receptors on platelet surface.
- Carbenicillin indanyl is an orally active ester of carbenicillin, used for treatment of UTI caused by pseudomonas and proteus.
Penicillin is the metabolic product of ‑
| A |
Aminoadipic acid |
|
| B |
Aminocaproic acid |
|
| C |
Levulinic acid |
|
| D |
Arachidonic acid |
Penicillin is the metabolic product of ‑
| A |
Aminoadipic acid |
|
| B |
Aminocaproic acid |
|
| C |
Levulinic acid |
|
| D |
Arachidonic acid |
Ans. is ‘a’ i.e., Aminoadipic acid
Penicillin is a product of secondary metabolic pathway of Penicillium chrysogenum.
α-aminoadipic acid is the precursor of penicillin.
This compound is normally converted to lysine via primary metabolic pathway.
However, when the growth of fungus is inhibited, a-aminoadipic acid is converted to penicillin via secondary metabolic pathway.
Which among the following is the drug of choice for the micro-organism shown in the photomicrograph below? 
| A |
Penicillin G. |
|
| B |
Tetracycline. |
|
| C |
Azithromycin. |
|
| D |
Doxycycline. |
Which among the following is the drug of choice for the micro-organism shown in the photomicrograph below?
| A |
Penicillin G. |
|
| B |
Tetracycline. |
|
| C |
Azithromycin. |
|
| D |
Doxycycline. |
Ans:A.)Penicillin G.
The micro-organism shown in the photomicrograph above represents Treponema pallidum.
Treponema pallidum.
- Treponema pallidum is a Gram-negative bacteria which is spiral in shape.
- It is an obligate internal parasite which causes syphilis, a chronic human disease.
- Untreated syphilis progresses in a series of distinct stages (primary, secondary, latent, and tertiary.)
- Parenteral penicillin G remains the treatment of choice for syphilis (Treponema pallidum) and resistance to penicillin has not been reported.
- The following regimens are recommended for penicillin treatment:
- Primary or secondary syphilis – Benzathine penicillin G 2.4 million units intramuscularly (IM) in a single dose
- Early latent syphilis – Benzathine penicillin G 2.4 million units IM in a single dose
- Late latent syphilis or latent syphilis of unknown duration – Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals
True about Penicillin G
| A |
It can be given orally |
|
| B |
It is has broad spectrum activity |
|
| C |
Used for treatment rat bite fever |
|
| D |
Probenecid given along with PnG decrease its direction of action |
True about Penicillin G
| A |
It can be given orally |
|
| B |
It is has broad spectrum activity |
|
| C |
Used for treatment rat bite fever |
|
| D |
Probenecid given along with PnG decrease its direction of action |
Ans. c. Used for treatment of rat bite fever
Penicillin G is not given by oral route: (KDT 6/e p697)
- Penicillin G is acid labile, destroyed by gastric acid, so not given by oral route.
Penicillin G is not a broad spectrum antibiotic:
- Penicillin G is 13-lactam antibiotics and are used in the treatment of bacterial infections caused by susceptible, usually Gram-positive, organisms.
Penicillin G is DOC for: (KDT 6/e p699)
- Actinomycosis
- Trench mouth
Probenicid is given along with Penicillin G: (VDT 6/c p30)
- Increase its action because it has high affinity for the tubular OATP, so it blocks the transport of penicillin and increase its efficacy. (KDT 6/e p30)
- Decreases volume of distribution of penicillin G.
Penicillin G
- MOA: It inhibits cell wall synthesis b.y interfering with the transpeptidation reaction°.
- Penicillin G is fl-lactam antibiotics and are used in the treatment of bacterial infections caused by susceptible, usually Gram-positive, organisms°.
Resistance to penicillin G is due to 4 mechanism
- Inactivation of antibiotic by beta-lactamase: MC°
- Modification of target penicillin binding protein (PBP)Q
- Impaired penetration of the drug to target PBPQ Efflux°
Penicillin G is DOC for: (KDT 6/e p699)
- Anthrax’
- Actinomycosis°
- Trench mouth
- Rat bite feverQ
- Probenicid is given along with Penicillin G, increase its action because it has high affinity for the tubular OATP, so it blocks the transport of penicillin and increase its efficacy°. (KDT 6/e p30)
- Probenicid also decreases volume of distribution of penicillin G°.
A young man presents with asymptomatic macules and erythematous painless lesion over glans with generalised lymphadenopathy. Treatment of choice in this condition:
| A |
Ceftriaxone |
|
| B |
Benzathine penicillin |
|
| C |
Acyclovir |
|
| D |
Fluconazole |
A young man presents with asymptomatic macules and erythematous painless lesion over glans with generalised lymphadenopathy. Treatment of choice in this condition:
| A |
Ceftriaxone |
|
| B |
Benzathine penicillin |
|
| C |
Acyclovir |
|
| D |
Fluconazole |
Ans. b. Benzathine penicillin
A 25-year-old person with history of repeated episodes of Rheumatic fever is hypersensitive to penicillin. Which of the following drug can be prescribed to him
| A |
Penicillin G |
|
| B |
Sulfisoxazole |
|
| C |
Sulfasalazine |
|
| D |
Streptomycin |
A 25-year-old person with history of repeated episodes of Rheumatic fever is hypersensitive to penicillin. Which of the following drug can be prescribed to him
| A |
Penicillin G |
|
| B |
Sulfisoxazole |
|
| C |
Sulfasalazine |
|
| D |
Streptomycin |
Ans. b. Sulfisoxazole
Which of the followi ‘s true about Penicillin G?
| A |
Broad spectrum |
|
| B |
It is effective orally |
|
| C |
Used for treatment of rat bite fever |
|
| D |
Probenecid given along with Penicillin G decreases duration of its action |
Which of the followi ‘s true about Penicillin G?
| A |
Broad spectrum |
|
| B |
It is effective orally |
|
| C |
Used for treatment of rat bite fever |
|
| D |
Probenecid given along with Penicillin G decreases duration of its action |
Ans. c. Used for treatment of rat bite fever
Penicillin G is not given by oral route:
- Penicillin G is acid labile, destroyed by gastric acid, so not given by oral route.
- Low oral bioavailability (only useful parenterally)
Penicillin C is not a broad-spectrum antibiotic:
- Penicillin G is 0-lactam antibiotics and is used in the treatment of bacterial infections caused by susceptible, usually Gram-positive, organisms.
- Narrow spectrum
Penicillin G is DOC for:
- Anthrax
- Actinomycosis
- Trench mouth
- Rat bite fever
Probenecid is given along with Penicillin G:
- Increase its action because it has high affinity for the tubular OATP, so it blocks the transport of penicillin and increase its efficacy.
- Decreases volume of distribution of penicillin G.
Penicillin G
- MOA: It inhibits cell synthesis by interfering with the transpeptidation reactions
- Penicillin G is 13-lactam antibiotics and is used in the treatment of bacterial infections caused by suscptible usually Gram-positive organismsQ.
- Resistance to penicillin G is due to 4 mechanism
- Inactivation of antibiotic by beta-lactamase: MCQ
- Modification of target penicillin binding protein (PBP)Q
- Impaired penetration of the drug to target PQ
- EffluxQ
- Pharmacokinetics: enicillin G is acid labile, destroyed by gastric acid, so not given by oral routes
- Probenecid is given along with Penicillin G, increase its action because it has high affinity for the tubular OATP,
- so it blocks the transport of penicillin and increase its efficacyQ.
- Probenecid also decreases volume of distribution of penicillin Gs.
In G6PD deficiency hemolysis can be caused byall except ‑
| A |
Chloroquine |
|
| B |
Primaquine |
|
| C |
Quinine |
|
| D |
Penicillin |
In G6PD deficiency hemolysis can be caused byall except ‑
| A |
Chloroquine |
|
| B |
Primaquine |
|
| C |
Quinine |
|
| D |
Penicillin |
Ans. is ‘d’ i.e., Penicillin
Which of the following is antipseudomonal penicillin ‑
| A |
Cephalexin |
|
| B |
Cloxacillin |
|
| C |
Piperacillin |
|
| D |
Dicloxacillin |
Which of the following is antipseudomonal penicillin ‑
| A |
Cephalexin |
|
| B |
Cloxacillin |
|
| C |
Piperacillin |
|
| D |
Dicloxacillin |
Ans. is ‘c’ i.e., Piperacillin
Drugs acting against Pseudomonas.
- Penicillins – Piperacillin, Carbenicillin, Ticarcillin, Mezlocillin.
- Cephalosporins – Ceftazidime, Cefoperazone, Cefepime.
- Carbapenems – Imipenem, meropenem
- Monobactams – Aztreonam.
- Aminoglycosides – Tobramycin, Gentamycin, Amikacin.
- Fluroquinolones – Ciprofloxacin, Levofloxacin, Norfloxacin..
- Other – Polymixin B, Colistin.
- For most of the infection of pseudomonas, treatment of choice is the combination of an antipseudomonal 13-lactam and an aminoglycoside.
All of the following are therapeutic uses of penicillin G, except
| A |
Bacterial meningitis |
|
| B |
Rickettsial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
All of the following are therapeutic uses of penicillin G, except
| A |
Bacterial meningitis |
|
| B |
Rickettsial infection |
|
| C |
Syphilis |
|
| D |
Anthrax |
Ans. is ‘b’ i.e., Rickettsial infection
Antibacterial spectrum of Penicillin G (Benzvl
- PnG is a narrow spectrum antibiotic
- Activity is limited primary to gram positive bacteria (and few others).
- Amongst gram negative organisms, penicillin has activity against gonococci, meningococci, few Ecoli & proteus.
- Majority of gram negative bacilli are insensitive.
- M. Tuberculosis, Ricketsiae, chlamydia, protozoa, fungi and viruses are totally insensitive to penicillin G.
Penicillin G is the DOC for (Laurence 9thie 218. Katzung 7301
|
1. |
Meningococcal meningitis |
7. |
Leptospira |
|
2. |
Bacillus anthracis (anthrax) |
8. |
Actinomyces israelii (Actinomycosis) |
|
3. |
Clostridium perfringens (gas gangrene) |
9. |
Borrel i a burgdorferi (Lyme disease) |
|
4. |
Clostridium tetani (tetanus) |
10. |
Enterococci |
|
5. |
Corynebacterium diphtheriae |
11. |
Streptococci |
|
6. |
Treponema pallidum (syphilis) |
12. |
Susceptible pneumococci |
