
PRIMITIVE REFLEXES
| A | Normal child | |
| B | Brain damage | |
| C | Irritable child | |
| D | Hungry child |
| A | Normal child | |
| B | Brain damage | |
| C | Irritable child | |
| D | Hungry child |
MORO REFLEX is also known as embrace reflex or startle reflex. It is a reflex seen in infants in response to stimuli, e.g. that produced by suddenly striking the surface on which the infant rests. To elicit this reflex the head is momentarily allowed to fall back and then is re supported by the examiner’s hand. The child symmetrically abducts and extends the arms, flexes the thumbs. This movement is followed by flexion and adduction of upper extremities. Persistence of Moro’s reflex beyond 12 weeks indicates neurological damage.
Examination of a 6-hour-old infant delivered with difficulty by low forceps reveals an asymmetric Moro reflex involving the right arm. Infant is cyanotic and has labored respiration. Abdomen does not bulge with inspiration, and there are decreased breath sounds in the right chest. Most likely diagnosis is?
| A |
Respiratory distress syndrome |
|
| B |
Meconium aspiration syndrome |
|
| C |
Ipsilateral paralysis of the diaphragm |
|
| D |
Tracheoesophageal fistula |
Examination of a 6-hour-old infant delivered with difficulty by low forceps reveals an asymmetric Moro reflex involving the right arm. Infant is cyanotic and has labored respiration. Abdomen does not bulge with inspiration, and there are decreased breath sounds in the right chest. Most likely diagnosis is?
| A |
Respiratory distress syndrome |
|
| B |
Meconium aspiration syndrome |
|
| C |
Ipsilateral paralysis of the diaphragm |
|
| D |
Tracheoesophageal fistula |
Ans:C.)Ipsilateral paralysis of the diaphragm .
- Phrenic nerve injury with ipsilateral diaphragmatic paralysis must be suspected in this infant.
- The abdomen does not bulge with the breathing is mostly thoracic.
- Diagnosis is made during fluoroscopy, Respiratory distress syndrome is more seen in preterm infants and presents with cyanosis, tachypnea and grunting respirations.
- The mother usually has a history of difficult delivery.
- Chest x-ray reveals a ground-glass appearance. Meconium aspiration syndrome appears at birth, usually in term or post-term infants.
- There is a history of meconium-stained amniotic fluid. When meconium is aspirated into the lungs, respiratory distress may occur within the first hours of life.
- Overdistention of the chest may be present. Meconium aspiration syndrome is not associated with an asymmetric Moro reflex.
- Tracheoesophageal fistula presents as choking and cyanosis with feeding.
- It should be suspected in cases of maternal polyhydramnios, or excessive oral secretions of the infant.
- Choanal atresia is suspected in a cyanotic newborn who becomes pink on crying, and the diagnosis is made by failure to pass a catheter through the nasal passages.
| A | The sequence and time of attainment of milestones may vary among individual children | |
| B | Development always proceeds in a cephalocaudal sequence | |
| C | Presence of primitive reflexes is essential for attaining voluntary actions | |
| D | All of the above |
| A | The sequence and time of attainment of milestones may vary among individual children | |
| B | Development always proceeds in a cephalocaudal sequence | |
| C | Presence of primitive reflexes is essential for attaining voluntary actions | |
| D | All of the above |
All the four statements are correct. The attainment of milestones varies from one child to another. It differs amongst the brothers and sisters. This is because of different rate of myelination and development of the nervous system amongst different children. Development always proceeds in a cephalocaudal sequence. In the beginning there is head control. After this the child sits up and walking occurs after this.
Persistence of Moro’s reflex is abnormal beyond the age of
| A |
3rd month |
|
| B |
4th month |
|
| C |
5th month |
|
| D | 6th month |
Persistence of Moro’s reflex is abnormal beyond the age of
| A |
3rd month |
|
| B |
4th month |
|
| C |
5th month |
|
| D | 6th month |
3rd month [Ref. Ghai 6th/e p 146, Nelson 176Ve p 1979; Neurology of the newborn p. 133, Nov 08] According to Ghai 6th/e p. 146
“Moro’s reflex disappear at three month of age and persistence of this reflex beyond three months is abnormal.” According to Ghai 7m/e p. 114
“Moro’s reflex disappear by six months in normal infant”
We have done an extensive search for this one. We are sure of one point.
Persistence of Moro’s reflex beyond 6 months of age indicates neurological abnormality
“In the normal infant the 17101–0‘ s reflex begins to fade at three months of age and gradually disappear at 4-6 months of age. When it persist beyond 6 months of age it indicates delay in CNS development such as cerebral palsy.”
(Tachdjian clinical paediatric orthopaedic p. 371)
But still we are not sure what would be the answer for
Moro’s reflex disappear at ??
Moro’s reflex is abnormal after:
| A |
4 weeks |
|
| B |
10 weeks |
|
| C |
12 weeks |
|
| D |
20-weeks |
Moro’s reflex is abnormal after:
| A |
4 weeks |
|
| B |
10 weeks |
|
| C |
12 weeks |
|
| D |
20-weeks |
- Grasp reflex: It is usually present in neonate and may persist upto 6months.
- Placing/stepping reflex: This neonatal reflex disappears after 6weeks.
- Asymmetric tonic neck reflex: Obligatory fixed ATNR beyond 4months of age is abnormal and precludes the ability to roll over.
- Side protective reflex: Emerges after 5months of age.
- Parachute reflex: It emerges at 7-8 months and is well developed by 10-12months.
Persistant Moro’s reflex at 6-7 months indicates ‑
| A |
Normal child |
|
| B |
Brain damage |
|
| C |
Hungry child |
|
| D |
Irritable child |
Persistant Moro’s reflex at 6-7 months indicates ‑
| A |
Normal child |
|
| B |
Brain damage |
|
| C |
Hungry child |
|
| D |
Irritable child |
Ans. is ‘b’ i.e., Brain damage
Moro’s Reflex disappears at-
| A |
3 months |
|
| B |
5 months |
|
| C |
6 months |
|
| D |
7 months |
Moro’s Reflex disappears at-
| A |
3 months |
|
| B |
5 months |
|
| C |
6 months |
|
| D |
7 months |
Ans. is `c’ i.e., 6 months
Also know
Rooting reflex
o When mother’s breast touches the baby’s upper lip or the side of mouth, the baby opens his mouth and searches for the nipple with an open mouth.
Sucking reflex
o Stimulation of the upper and lower lips produces movement of the lip and tongue in the direction of the stimulus. Swallowing reflex
o When the mouth is filled with milk, the baby swallows the milk and then breathes.
All these three reflexes appear at 32 weeks of gestation and becomes less prominent after 1 month of birth.
Atypical moro’s reflex is seen in A/E –
| A |
# clavicle |
|
| B |
Sternomastoid tumor |
|
| C |
Shoulder dislocation |
|
| D |
Brachial plexus injury |
Atypical moro’s reflex is seen in A/E –
| A |
# clavicle |
|
| B |
Sternomastoid tumor |
|
| C |
Shoulder dislocation |
|
| D |
Brachial plexus injury |
Ans. is ‘b’ i.e., Sternomastoid tumour
Identify the reflex shown in the picture below ? 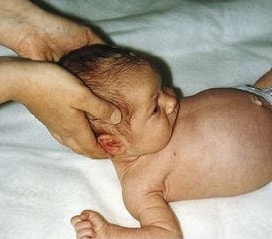
| A |
Moro reflex. |
|
| B |
Grasp reflex. |
|
| C |
Galant’s infantile reflex. |
|
| D |
None. |
Identify the reflex shown in the picture below ?
| A |
Moro reflex. |
|
| B |
Grasp reflex. |
|
| C |
Galant’s infantile reflex. |
|
| D |
None. |
- The Moro reflex, as shown in the picture above evaluates vestibular maturation and the relationship between flexor and extensor tone.
- Elicitation of the reflex involves a short (10 cm), sudden drop of the head when the infant is supine.
- The full response involves extension of the arms, “fanning” of the fingers, and then upper extremity flexion followed by a cry.
- An incomplete but identifiable reflex becomes apparent at approximately 32 weeks’ gestation, and by 38 weeks it is essentially complete.
- Very immature infants demonstrate extension of the arms and fingers but do not show true flexion or make a sustained cry.
- Marked asymmetry of response may be associated with focal neurologic impairment.
Asymmetric Moro’s reflex at birth is indicative of:
| A |
HIE |
|
| B |
Brain damage |
|
| C |
Erb’s palsy |
|
| D |
Kernicterus |
Asymmetric Moro’s reflex at birth is indicative of:
| A |
HIE |
|
| B |
Brain damage |
|
| C |
Erb’s palsy |
|
| D |
Kernicterus |
Ans. c. Erb’s palsy
