Sigmoid Volvulus
Coffee bean sign is seen in?
| A | Gastric volvulus | |
| B |
Sigmoid volvulus |
|
| C | Hypertrophic pyloric stenosis | |
| D |
Midgut volvulus |
Coffee bean sign is seen in?
| A | Gastric volvulus | |
| B |
Sigmoid volvulus |
|
| C | Hypertrophic pyloric stenosis | |
| D |
Midgut volvulus |
Sigmoid volvulus REF: Wofganag 5th e p. 846/748
|
Sign |
Disease |
|
Rat tail appearance |
Carcinoma esophagus |
|
Bird beak appearance |
Achalasia |
|
Beak sign/double track/ tram track |
Hypertrophic pyloric stenosis |
|
Medusa head colonies on CT |
Round worm |
|
Pincer/claw/coiled spring/target/meniscus sign |
Intussception |
|
Coffee bean sign |
Sigmoid volvulous |
|
Lead pipe appearance |
Ulcerative colitis |
|
String of kantor/bull’s eye |
Chron’s disease |
|
Thumb printing sign |
Ischemic colitis |
|
Saw tooth appeance on barium enema |
Diverticulosis |
|
Apple core sign |
Carcinoma colon |
|
Cork screw appearance |
Diffuse esophageal spasm |
|
String sign |
Hypertrophic pyloric stenosis |
in
| A | Right iliac fossa | |
| B | Left iliac fossa | |
| C | Lt. hypochondrium | |
| D | Rt. Hypochondrium |
in
| A | Right iliac fossa | |
| B | Left iliac fossa | |
| C | Lt. hypochondrium | |
| D | Rt. Hypochondrium |
Plain Xray abdomen finding in Sigmoid Volvulus
1. Characteristic bent inner tube or coffee bean appearance with convexity of loop lying in the right upper quadrant (opposite to the site of obstruction)
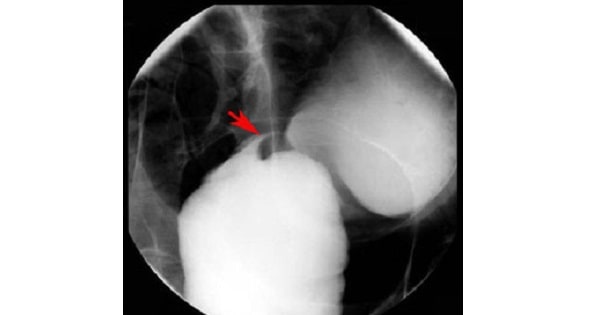
2. Contrast study (gastrografin enema) – bird beak appearance i.e. narrowing at the site of voivulus.
Bird of Prey” sign is seen in the radiographic barium examination of:
| A | Gastric volvulus | |
| B | Intussusception | |
| C | Sigmoid volvulus | |
| D | Caeca! volvulus |
Bird of Prey” sign is seen in the radiographic barium examination of:
| A | Gastric volvulus | |
| B | Intussusception | |
| C | Sigmoid volvulus | |
| D | Caeca! volvulus |
Sigmoid volvulus
| A | Gastric volvulus | |
| B | Intussusception | |
| C | Sigmoid volvulus | |
| D | Cecal volvulus |
| A | Gastric volvulus | |
| B | Intussusception | |
| C | Sigmoid volvulus | |
| D | Cecal volvulus |
Sigmoid volvulus
A patient with abdominal pain shows “coffee bean” sign in plain abdominal X-ray. He probably have:
| A |
Colon carcinoma |
|
| B |
Duodenal atresia |
|
| C |
Acute pancreatitis |
|
| D |
Sigmoid volvulus |
A patient with abdominal pain shows “coffee bean” sign in plain abdominal X-ray. He probably have:
| A |
Colon carcinoma |
|
| B |
Duodenal atresia |
|
| C |
Acute pancreatitis |
|
| D |
Sigmoid volvulus |
Sigmoid volvulus is a closed-loop colonic obstruction due to twisting along the mesenteric or long axis of the bowel.
Although colonic volvulus is not common, about 90% of cases occur in the sigmoid colon.
On plain abdominal films, the sigmoid volvulus forms an inverted U-shaped structure with the twisted sigmoid loops lying adjacent and having an oval appearance called the “coffee bean” sign.
On barium enema examination, tapered obstruction of the sigmoid colon is found.
Ref: Ott D.J. (2011). Chapter 10. Gastrointestinal Tract. In M.Y. Chen, T.L. Pope, D.J. Ott (Eds), Basic Radiology, 2e.
Which of the following statement about volvulus is false?
| A |
More common in psychiatric patients |
|
| B |
Sigmoid volvulus is more common than caecal volvulus |
|
| C |
Lower GI scopy is contraindicated in sigmoid volvulus |
|
| D |
Volvulus of caecum is managed by conservative methods |
Which of the following statement about volvulus is false?
| A |
More common in psychiatric patients |
|
| B |
Sigmoid volvulus is more common than caecal volvulus |
|
| C |
Lower GI scopy is contraindicated in sigmoid volvulus |
|
| D |
Volvulus of caecum is managed by conservative methods |
A volvulus is the twisting strangulation of an intestinal segment around an axis which is formed by an axis or an adhesion.
What is the definitive treatment of sigmoid volvulus?
| A |
Surgical correction |
|
| B |
Colectomy |
|
| C |
Enema |
|
| D |
Endoscopic correction |
What is the definitive treatment of sigmoid volvulus?
| A |
Surgical correction |
|
| B |
Colectomy |
|
| C |
Enema |
|
| D |
Endoscopic correction |
“Definitive treatment of sigmoid volvulus is sigmoid colectomy”
- Unless there are obvious signs of gangrene or peritonitis, the initial management of sigmoid volvulus is resuscitation followed by endoscopic decompression (by using rigid proctosigmoidoscopy or flexible sigmoidoscopy or colonoscopy) ; a rectal tube is inserted and kept to maintain decompression. Endoscopic decompression is contraindicated if there is evidence of strangulation or perforation.
- Although endoscopic decompression is successful in majority of patients, recurrence rate is quite high. Therefore elective sigmoid colectomy is performed as the definitive procedure after the patient is stabilized and adequate bowel preparation done.
- Emergency laparotomy is performed if strangulation or perforation is suspected or if attempts of endoscopic decompression fail.
Rotation of sigmoid volvulus occur in which direction?
| A |
Clockwise |
|
| B |
Anticlockwise |
|
| C |
Initially clockwise later anticlockwise |
|
| D |
Either clockwise or anticlockwise |
Rotation of sigmoid volvulus occur in which direction?
| A |
Clockwise |
|
| B |
Anticlockwise |
|
| C |
Initially clockwise later anticlockwise |
|
| D |
Either clockwise or anticlockwise |
“Rotation in sigmoid volvulus nearly always occur in anticlockwise direction”
- Sigmoid volvulus ——— Anticlockwise
- Cecal volvulus ———– Clockwise
Which of the following doesn’t present with bleeding per rectum?
| A |
Ca rectum |
|
| B |
Sigmoid volvulus |
|
| C |
Inflammation of Meckel’s diverticulum |
|
| D |
Enteric fever |
Which of the following doesn’t present with bleeding per rectum?
| A |
Ca rectum |
|
| B |
Sigmoid volvulus |
|
| C |
Inflammation of Meckel’s diverticulum |
|
| D |
Enteric fever |
Sigmoid volvulus presents with features of lower intestinal obstruction not bleeding per rectum. Volvulus refers to torsion of a segment of the alimentary tract, which often leads to bowel obstruction. The most common sites of volvulus are the sigmoid colon and cecum.
Commonest site of volvulus is:
| A |
Proximal jejunum |
|
| B |
Stomach |
|
| C |
Cecum |
|
| D |
Sigmoid |
Commonest site of volvulus is:
| A |
Proximal jejunum |
|
| B |
Stomach |
|
| C |
Cecum |
|
| D |
Sigmoid |
Ans is ‘d’ i.e. Sigmoid
Which of the following statement about volvulus is False:
| A |
More common in psychiatric patients |
|
| B |
Sigmoid volvulus is more common than caecal volvulus |
|
| C |
Lower GI scopy is contraindicated in sigmoid volvulus |
|
| D |
All |
Which of the following statement about volvulus is False:
| A |
More common in psychiatric patients |
|
| B |
Sigmoid volvulus is more common than caecal volvulus |
|
| C |
Lower GI scopy is contraindicated in sigmoid volvulus |
|
| D |
All |
Ans is ‘c” i.e. Lower GI scopy is contraindicated in sigmoid volvulus
- Volvulus describes a condition in which there is rotation of a segment of the intestine on an axis formed by its mesentery resulting in partial or complete obstruction of the lumen and may be followed by circulatory impairment of the bowel.
- Most common site is colon, among which following are involved in descending order – Sigmoid volvulus (- 75%)
– Cecal volvulus (< 25%)
– Transverse colon
– Splenic flexure
– Sigmoid volvulus
- Most common site of volvulus
- Volvulus can occur in any segment of large bowel that is attached to a long and floppy mesentery that is fixed to the
retroperitoneum by a narrow base of origin. The mesenteric anatomy is such that volvulus is most commonly seen in sigmoid colon.
- Associated predisposing factors are :
– age : average age of presentation is 60-70 yrs. – chronic constipation
– institutionalized or neurologically impaired or psychiatric patients (their medication may decrease intestinal
motility, or they may fail to pass stool regularly, leading to fecal loaded large bowel predisposing to volvulus) – diet high in fibre and vegetables (as in third world countries)
- Signs and symptoms are those of acute or subacute intestinal obstruction.
- X-ray picture is dramatic
– there is a markedly dilated sigmoid colon with the appearance of a bent inner tube or coffee bean appearance. Inferior convergence of the dilated loop points towards left side of pelvis.
– contrast enema demonstrates the point of obstruction with the pathognomic ‘birds beak’ or ‘bird of prey’ or ‘ace of spades’ sign.
- Management of sigmoid volvulus
- Unless there are obvious signs of gangrene or peritonitis, the initial management is resuscitation followed by endoscopic decompression and detorsion.
- Decompression/detorsion can be achieved by placement of rectal tube through a proctoscope or the use of a colonoscope.
- If detorsion / decompression cannot be achieved with either the rectal tube or colonoscope, laprotomy with resections of the sigmoid colon is done.
- Even if detorsion of the sigmoid volvulus is successful, risk of recurrence is high (approx. 50%). Hence an effective sigmoid colectomy is indicated after the pt. has stabilized.
- Any evidence of bowel gangrene or perforation contraindicates non-operative decompression and an immediate surgical exploration is done.
Cecal volvulus
The condition commonly referred to as cecal volvulus is actually a cecocolic volvulus and consists of an axial rotation of the terminal ileum, cecum and ascending colon.
- Cecal bascule – is a condition in which the cecum folds in a cephalad direction anteriorly over a fixed ascending colon. This causes intermittent bouts of abdominal pain because the mobile cecum causes intermittent episodes of Isolated cecal obstruction. It is relieved spontaneously as the cecum falls back into its normal position.
- Cecocolic volvulus is possible because of lack of fixation of the cecum to the retroperitoneum.
- Associate predisposing factors are:
– previous surgery
– pregnancy
– malrotation
– obstructing lesion of the left colon
- Cecocolic volvulus affects a younger age group (late 50s) than sigmoid volvulus (60s & 70s).
- X-ray picture
– dilated cecum usually occupying the left upper quadrant.
– haustral markings can be seen in the distended cecocolic segment and is a distinguishing feature from sigmoid colon in which generally there are no haustra.
- Management
- According to Schwartz Surgery – Cecal volvulus, unlike sigmoid volvulus can almost never be detorsed / decompressed endoscopically. As vascular compromise occurs early in the course of cecal volvulus, surgical exploration is necessary when the diagnosis is made. Right hemicolectomy is the procedure of choice.
- Sabiston surgery writes that – ‘Although there have been reports of detorsion of cecocolic volvulus with a colonoscope most cases require operation to correct the volvulus and prevent ischemia.”
An article published in the journal ‘Diseases of Colon and Rectum’ – The management of Cecal Volvulus writes“Non-operative decompression of cecal volvulus is rarely achievable”
Definitive treatment of sigmoid volvulus is‑
| A |
Surgical correction |
|
| B |
Colectomy |
|
| C |
Enema |
|
| D |
Endoscopic correction |
Definitive treatment of sigmoid volvulus is‑
| A |
Surgical correction |
|
| B |
Colectomy |
|
| C |
Enema |
|
| D |
Endoscopic correction |
Ans ‘b’ Colectomy
- The definitive treatment of sigmoid volvulus is sigmoid colectomy.
- Management of sigmoid volvulus
- Unless there are obvious signs of gangrene or peritonitis, the initial management of sigmoid volvulus is resucitation followed by endoscopic decompression (by using rigid proctosigmoidoscope or flexible sigmoidoscope or colonoscope); a rectal tube is inserted and kept to maintain decompression) Endoscopic decompression is contraindicated if there is evidence of strangulation or perforation.
- Although endoscopic decompression is susccessful in majority of patients, recurrence rate is quite high. Therefore elective sigmoid colectomy is performed as the definitive procedure after the patient is stabilized and adequate bowel preparation done.
- Emergency Laparotomy is performed if strangulation or perforation is suspected or if attempts of endoscopic decompression fail.
Predisposing factors for sigmoid volvulus are ‑
| A |
Band of adhesion |
|
| B |
Long pelvic meso colon |
|
| C |
Narrow attachment of pelvic mesocolon |
|
| D |
All of the above |
Predisposing factors for sigmoid volvulus are ‑
| A |
Band of adhesion |
|
| B |
Long pelvic meso colon |
|
| C |
Narrow attachment of pelvic mesocolon |
|
| D |
All of the above |
Ans. is ‘d’ i.e., All of the above
Rotation of sigmoid volvulus occurs-
| A |
Clockwise |
|
| B |
Anticlockwise |
|
| C |
Initially clockwise later anticlockwise |
|
| D |
Either clockwise or anticlockwise |
Rotation of sigmoid volvulus occurs-
| A |
Clockwise |
|
| B |
Anticlockwise |
|
| C |
Initially clockwise later anticlockwise |
|
| D |
Either clockwise or anticlockwise |
Ans is ‘b’ i.e. Anticlockwise
“Rotation in Sigmoid Volvulus nearly always occur in the anticlockwise direction”- Bailey & Love Remember
Sigmoid Volvulus—Anticlockwise
Cecal Volvulus —— Clockwise
Sigmoid volvulus rotation occurs –
| A |
Clockwise |
|
| B |
Anticlock wise |
|
| C |
Both clock wise and anti clock wise |
|
| D |
Axial in direction |
Sigmoid volvulus rotation occurs –
| A |
Clockwise |
|
| B |
Anticlock wise |
|
| C |
Both clock wise and anti clock wise |
|
| D |
Axial in direction |
Ans. is ‘b’ i.e., Anticlock wise
Bleeding per rectum is present in all, except ‑
| A |
Meckel’s diverticulum |
|
| B |
Sigmoid volvulus |
|
| C |
Carcinoma rectum |
|
| D |
Ulcerative colitis |
Bleeding per rectum is present in all, except ‑
| A |
Meckel’s diverticulum |
|
| B |
Sigmoid volvulus |
|
| C |
Carcinoma rectum |
|
| D |
Ulcerative colitis |
Ans. is `b’ i.e., Sigmoid Volvulus
Volvulus does not cause bleeding
|
Causes of lower G.I. bleeding |
|
|
|
A) Common |
B) Less common |
C) Rare |
|
Angiodysplasia |
Neoplasia —> Carcinoma, polyps |
Meckel’s diverticulum |
|
Diverticulitis |
Colitis –> Radiation, Ischaemic, Ulcerative |
Intussusception |
|
Anorectal disease |
Infective –> Enteric fever, Amoebic ulcer, T.B. |
|
|
(Hemorrhoids, Anal fissure) |
HIV related (Gonorrhoea, C.M.V.) |
|
Most common site of volvulus is:
March 2010 September 2010
| A |
Ileum |
|
| B |
Appendix |
|
| C |
Sigmoid colon |
|
| D |
Caecum |
Most common site of volvulus is:
March 2010 September 2010
| A |
Ileum |
|
| B |
Appendix |
|
| C |
Sigmoid colon |
|
| D |
Caecum |
Ans. C: Sigmoid colon
Volvulus refers to torsion of a segment of the alimentary tract, which often leads to bowel obstruction. The most common sites of volvulus am the sigmoid colon and cecum.
In sigmoid volvulus, rotation nearly occurs in the anticlockwise direction.
Volvulus of other portions of the alimentary tract, such as the stomach, gallbladder, small bowel, splenic flexure, and transverse colon, are rare
Predisposing factors includes a high residue diet and constipation.
A plain abdominal X-ray in a patient with a sigmoid volvulus will show a distended bowel loop with its apex
in ?
| A |
Right iliac fossa |
|
| B |
Left iliac fossa |
|
| C |
Lt. hypochondrium |
|
| D |
Rt. Hypochondrium |
A plain abdominal X-ray in a patient with a sigmoid volvulus will show a distended bowel loop with its apex
in ?
| A |
Right iliac fossa |
|
| B |
Left iliac fossa |
|
| C |
Lt. hypochondrium |
|
| D |
Rt. Hypochondrium |
Plain Xray abdomen finding in Sigmoid Volvulus
1. Characteristic bent inner tube or coffee bean appearance with convexity of loop lying in the right upper quadrant (opposite to the site of obstruction)
2. Contrast study (gastrografin enema) – bird beak appearance i.e. narrowing at the site of voivulus.
|
“Definitive treatment of sigmoid volvulus is sigmoid colectomy” Management of sigmoid volvulus
|
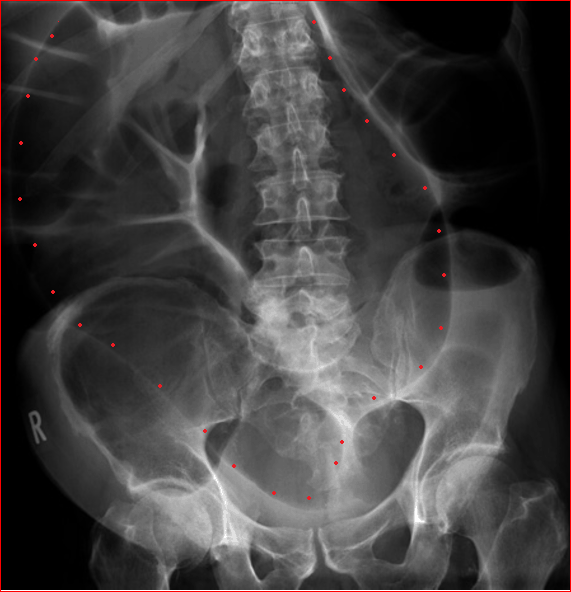
A patient presented with complain of abdominal pain,distension and absolute constipation.Abdominal X ray shows the following features.What can be the most probable diagnosis?
| A |
Colitis |
|
| B |
Paralytic Ileus |
|
| C |
Sigmoid Volvulus |
|
| D |
Cecal Volvulus |
A patient presented with complain of abdominal pain,distension and absolute constipation.Abdominal X ray shows the following features.What can be the most probable diagnosis?
| A |
Colitis |
|
| B |
Paralytic Ileus |
|
| C |
Sigmoid Volvulus |
|
| D |
Cecal Volvulus |
Ans:C.)Sigmoid Volvulus.
Abdominal X ray in the image shows the features of Sigmoid Volvulus
- The sigmoid colon is very dilated because it is twisted at the root of its mesentery in the left iliac fossa (LIF). The proximal large bowel is also dilated .
- The twisted loop of sigmoid colon is said to resemble a coffee bean.(marked by red dots) .
Twisting of the bowel – or ‘volvulus’ – is a specific cause of bowel obstruction.
- The two commonest types of bowel twisting are sigmoid volvulus and caecal volvulus.
Sigmoid volvulus
- The sigmoid colon is more prone to twisting than other segments of the large bowel because it is ‘mobile’ on its own mesentery, which arises from a fixed point in the left iliac fossa (LIF).
- Twisting at the root of the mesentery results in the formation of an enclosed loop of sigmoid colon which becomes very dilated.
- If untreated this can lead either to perforation, due to excessive dilatation, or to ischaemia due to compromise of the blood supply.
