
BETA ADRENERGIC RECEPTOR ANTAGONIST / BETA-BLOCKERS
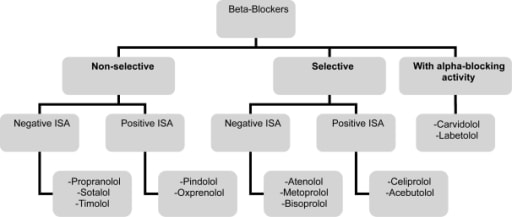
CLASSIFICATION:
EFFECTS:
- Beta-blockers have common effects and particular effects.
Common effects
- The effects of beta-blockers are primarily cardiovascular.
- Slow heart rate by ↓slope of slow diastolic depolarization and constitute group II of antiarrhythmic drugs.
- ↓ heart oxygen requirement, preventive treatment of angina pectoris.
- ↓ pathological arterial hypertension,
- ↓ cardiac output,
- ↓ renin secretion,
- ↓ sympathetic tone by a central effect.
- Beta-blockers ↓intraocular pressure by decreasing aqueous humor secretion.
Particular effects
- Beta-mimetic activity or intrinsic sympathomimetic activity or ISA.
- True beta-blockers – Prevent endogenous catecholamines from inducing beta effects.
Beta-1 receptors blocker – Cardioselective/selective β1/II generation beta blockers:
- Preferred in diabetes mellitus , bronchial asthma, peripheral vascular disease & hyperlipidemia.
Nebivolol –
- NO-mimetic vasodilatator effect.
- Most cardioselective.
Beta blockers with membrane-stabilizing effect:
- Exhibits “Local anesthetic or antiarrhythmic effect” by reducing transmembrane ion exchanges.
- Due to decreased depolarization rate by sodium entry.
- Should be avoided in Glaucoma – Risk of corneal anaesthesia.
- Pindolol, Acebutolol, Carvedilol, Betaxolol, Propranolol, Metoprolol & Labetalol.
- Propranolol inhibits transport of iodine in thyroid follicle.
- Carvedilol would have, at least in vitro, antioxydant properties.
PHARMACOKINETICS:
Acts by being liposoluble & water-soluble drugs.
- Liposoluble beta-blockers (propranolol & oxyprenolol):
- Quickly and completely absorbed by the digestive tract.
- Metabolized in liver and can undergo an inactivation known as first metabolism.
- Bound at 90% to plasma proteins.
- Great volume of distribution, i.e. they diffuse readily in tissues.
- Short duration of action (Esmolol)
- Short plasma half-life.
Water-soluble beta-blockers like atenolol, nadolol and sotalol:
- Less absorbed by digestive tract & more irregular way.
- Little metabolized by liver.
- Do not cross blood brain barrier.
- Not very bound to plasma proteins.
- Eliminated primarily by kidney in unchanged form – Hence, contraindicated in renal failure.
- Restricted volume of distribution.
- Long plasma half-life(Atenolol).
- Nadolol has longest half-life.
- Intermediate products such as pindolol & celiprolol.
- Labetalol has both alpha and & beta blocking action.
- Elimination in milk – Contraindicated during lactation.
USES:
Cardiovascular uses:
- Angina pectoris(unstable angina)
Tachycardia:
- Includes hyperthyroidic patients (Grave’s disease) taking propranolol.
- Arterial hypertension
- Myocardial infarction
Congestive heart failure
- Three beta-blockers having shown efficacy in this therapeutic use are
- Bisoprolol,
- Metoprolol
- Carvedilol.
Other therapeutic uses:
- Prevention of primary and secondary digestive bleeding in portal hypertension by rupture of esophageal varices(propranolol is usually used)
- Migraine, tremor, transitory somatic symptoms of anxiety, alcohol addiction in which there appears a beta overstimulation (propranolol is usually prescribed).
- Glaucoma – Primary open angle glaucoma.
- By ophthalmic solutions.
- Diffuses into general circulation causing adverse effects.
- Atherosclerosis
ADVERSE EFFECTS:
- Aggravation of congestive heart failure (with calcium channel blockers).
- Non-selective (Ist generation beta blockers) mask all effects of hypoglycemia Sweating, Palpitations, Dizziness.
- Congestive heart failure is both an indication & contraindication to beta-blockers use.
- Aggravation of bradyarrythmia; bradycardia, atrioventricular blocks.
- Beta-blockers like intrinsic sympathomimmetic activity like celiprolol, Oxprenolol, Pindolol, Pendutolol, Acebutolol, Alprenolol are useful.
- Due to partial agonistic activity apart from bloacking activity.
Masked hypoglycemic symptoms in diabetics:
- Tachycardia, sweating & tremors – Due to sympathetic stimulation acts as warning sings.
- Beta-blockers mask these symptoms (Except sweating) – Mediated via cholingeric system.
- Hence, patient directly fall into coma.
- Delayed recover from hypoglyβ1cemia – Due to β2 mediated hyperglycemia.
- Raised risk of developing type II diabetes after antihypertensive treatment.
Aggravation of asthmatic disease:
- Bronchoconstriction can occur due to β2 blockade.
- Causes hypotension, bradycardia, heart rhythm disorders & shock.
- Coldness of extremities.
- Worsened risk of anaphylactic shock.
Metabolic disorders:
- Increases triglycerides, cholesterol and VLDL (very low density lipoproteins).
Rebound of symptoms:
- Tachycardia, arterial hypertension, fainting, sweats, nervousness , especially risk of angina, myocardial infarction and sudden death.
- Diffusion in body after topical use of ophthalmic solutions elicit bradycardia, asthma, in elderly.
Various, rare disorders:
- Immunological disorders, lupus, fibroses.
CONTRAINDICATIONS :
- Decompensated CCF
- Bradycardia , HR< 60/min
- COPD
- Asthma
- Variant angina
- Carbohydrate intolerance
- Hyperlipidemia
- During lactation – Elimination in milk.
- Atherosclerosis
- Sick sinus syndrome
- Partial and complete heart block
- Raynaud’s disease –
- Due to vasoconstriction.
- Worsens peripheral vascular disease.
-
Sotalol is contraindicated in renal failure.
Exam Important
- Beta blockers are contraindicated in Decompensated CCF, Asthma , Atherosclerosis
- Beta blockers are antiarrhythmic agents TYPE II
- Acebutol, Atenolol & Metoprolol are cardioselective beta blocker
- Beta blockers are contraindicated in Asthma
- Atenolol is longer acting than metoprolol
- Labetalol has both alpha and & beta blocking action
- Nadolol has longest half life
- Sotalol is contraindicated in renal failure
- Beta blocker without local anaesthetic effect is Atenolol
- Beta blockers are contraindicated in Sick sinus syndrome
- Combination use of beta blockers and calcium channel blockers cause Heart block
- Contraindication of topical beta blockers asthma
- First line drug choice for management of hypertension in patients with angina Beta Blockers
- Effect of beta blocker’s on heart are Decrease in heart rate, Decreases cardiac output & Precipitates heart failure
- First line drug for primary open angle glaucoma is Beta blockers
- Shorest acting beta blocker Esmolol
- Mechanism of action of timolol is Nonselective beta blocker
- Beta blockers mask all effects of hypoglycemia Sweating, Palpitations, Dizziness
- Lipid insoluble beta blockers Are long acting
- Lipid insoluble beta blockers are Incompletely absorbed orally
- Lipid insoluble beta blockers Do not cross blood brain barrier
Don’t Forget to Solve all the previous Year Question asked on BETA ADRENERGIC RECEPTOR ANTAGONIST / BETA-BLOCKERS
