Growth Hormone
GROWTH HORMONE (GH)/SOMATOTROPIN
- Polypeptide.
- Synthesized & secreted by somatotropes.
- Subtype of acidophilic cells in adenohypophysis.
PHYSIOLOGICAL EFFECTS:
- Two major action –
- Stimulation of skeletal growth.
- Regulation of metabolism.
1. STIMULATION OF SKELETAL GROWTH:
- Mediated by “Somatomedins”/“Insulin-like Growth Factors” (IGF).
- Synthesized in liver.
- Somatomedin (IGF-1) stimulates proliferation of chondrocytes & osteocytes.
- Increases chondroitin sulfate deposition in cartilage.
- Increases ossification of newly formed cartilage.
CONDITIONS ASSOCIATED:
1. GH deficiency in early life –
- Causes dwarfism (reduced height).
- Yet, associated with Normal body proportion.
2. GH excess in early life –
- Leads to gigantism.
3. GH excess in adulthood –
- Results in Acromegaly.
2. REGULATION OF METABOLISM:
2a. On Protein metabolism:
- Predominantly anabolic effects on skeletal & cardiac muscle.
- By promoting amino acid transport into cells & Increasing protein synthesis.
2b. On Carbohydrate & Fat metabolism:
- Effects complicated by,
- Anti-insulin effect of GH.
- Insulin-like effects of somatomedins.
2c. Anti-insulin effects of GH –
- Decreased peripheral glucose utilization.
- Increased gluconeogenesis.
- Hyperglycemia.
- Lipolysis.
Conditions associated:
- “Insulin-Resistant Diabetes mellitus” –
- Caused by GH excess, (mainly by anti-insulin effects of GH).
2d. Insulin-like effects of somatomedins/IGF –
- Anti-lipolytic activity.
3. GH on kidneys:
- Promotes renal reabsorption of Ca2+, Na2+, K+& Cl–.
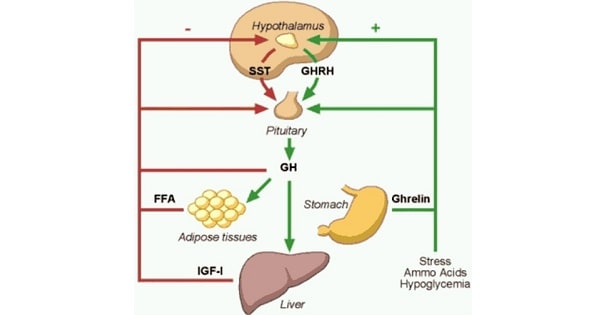
REGULATION:
- Regulated by hypothalamic GHRH.
- GH secreted in pulsatile fashion throughout life.
- Elevated secretion rate immediately after birth & at puberty.
- Large bursts of secretion at night during deep sleep onset.
FACTORS INFLUENCING GH SECRETION –
1. Stimuli increasing GH secretion –
- Hypoglycemia.
- Exercise.
- Fasting.
- Protein meals.
- Aminoacids (like arginine).
- Stress.
- Glucagon.
- Pyrogen.
- Lysin vasopressin.
- L-dopa & α-adrenergics.
- Estrogen & androgens.
- 2-deoxyglucose.
2. Stimuli decreasing GH secretion:
- REM sleep.
- Glucose.
- Somatostatin.
- Cortisol.
- FFA.
- GH itself decreases
- IGF- 1.
- Medroxyprogesterone.
Exam Question
GROWTH HORMONE
- Effect on skeletal growth mediated by “Somatomedins”/”Insulin-like Growth Factors” (IGF)
- GH, through somatomedin (IGF-1), stimulates proliferation of chondrocytes & osteocytes, resulting in increased chondroitin sulfate deposition in cartilage.
- Growth hormone excess in adulthood results in acromegaly.
- Anti-insulin effects due to the direct effect of GH include decreased peripheral utilization of glucose, increased gluconeogenesis & hyperglycemia.
- Insulin-like effects due to somatomedins(IGF) include “Anti-lipolytic” activity.
- GH is secreted in a pulsatile fashion.
- Large bursts of secretions occur at night during the onset of deep sleep.
- Stimuli increasing GH secretion – Exercise, hypoglycemia, fasting & stress.
- Stimuli decreasing GH secretion – REM sleep, Somatostatin & Cortisol.
- GH deficiency leads to “delayed fusion of epiphysis” – Ie., Proportionate dwarfism.
- Short stature, secondary to growth hormone deficiency is associated with “Normal body proportion”.
Don’t Forget to Solve all the previous Year Question asked on Growth Hormone