GROWTH HORMONE
Which among the following condition can cause an increase in growth hormone level in blood?
| A |
Hypoglycemia |
|
| B |
Cortisol |
|
| C |
Methylprednisolone |
|
| D |
Glucose |
Which among the following condition can cause an increase in growth hormone level in blood?
| A |
Hypoglycemia |
|
| B |
Cortisol |
|
| C |
Methylprednisolone |
|
| D |
Glucose |
Factors that stimulate secretion of growth hormone:
- Decreased blood glucose
- Decreased blood free fatty acids
- Starvation or fasting, protein deficiency
- Trauma, stress, excitement, exercise
- Testosterone, estrogen
- Deep sleep (stage II & IV)
- Growth hormone-releasing hormone
- Deoxyglucose
- Fasting
- Increase in circulating levels of few amino acids
- Glucagon
- Pyrogen
- Lysine vasopressin
- L-Dopa and adrenergic antagonists that penetrates the brain
- Apomorphine and other dopamine receptor agonists
- Increased blood glucose and free fatty acids
- Ageing and obesity
- Somatostatin
- Exogenous growth hormone
- Somatomedins (insulin-like growth factors)
- REM sleep
- Cortisol
- Medroxyprogesterone
At the cellular level the physiological affects of human growth hormone are mediated by?
| A |
Insulin |
|
| B |
Prolactin |
|
| C |
Somatotropin |
|
| D |
Insulin-like growth factors |
At the cellular level the physiological affects of human growth hormone are mediated by?
| A |
Insulin |
|
| B |
Prolactin |
|
| C |
Somatotropin |
|
| D |
Insulin-like growth factors |
Human growth hormone, also known as somatotropin is a 191 amino acid polypeptide with a molecular weight of 22,000 and is the major hormone regulating growth in humans. It is synthesized as a 28,000 Dalton precursor that is not biologically active. The gene for pre-growth hormone is found on chromosome 17. Growth hormone is part of a family of hormones which include prolactin and human placental lactogen.
Gluconeogensis affect A/E :
| A |
Lactate |
|
| B |
Glycerol |
|
| C |
Alanine |
|
| D |
Growth hormone |
Gluconeogensis affect A/E :
| A |
Lactate |
|
| B |
Glycerol |
|
| C |
Alanine |
|
| D |
Growth hormone |
D i.e. Growth hormone
A/E the following changes are seen on the 5th day of fasting:
| A |
Increase in FFA levels. |
|
| B |
Decreased glucose tolerance |
|
| C |
Decreased growth hormone |
|
| D |
Decreased level of Insulin |
A/E the following changes are seen on the 5th day of fasting:
| A |
Increase in FFA levels. |
|
| B |
Decreased glucose tolerance |
|
| C |
Decreased growth hormone |
|
| D |
Decreased level of Insulin |
C i.e. Decreased growth hormone
On 5th day of fasting, blood glucose level will be low and all the physiological changes will work in the direction of increasing the blood glucose level.
Acromegaly is due to excess of:
| A |
Somatomedin |
|
| B |
Growth hormone |
|
| C |
Somatostatin |
|
| D |
Insulin |
Acromegaly is due to excess of:
| A |
Somatomedin |
|
| B |
Growth hormone |
|
| C |
Somatostatin |
|
| D |
Insulin |
B i.e. Growth hormone
Tumors of somatortopes of the anterior pituitary secrete large amount of growth hormone, leading in children to gigantism and in adults to acromegaly.
Hypersecretion of GH is accompamied by hypersecretion of prolactin in 20 – 40% of patient with acromegaly.
Somatomedian: are polypeptide growth factors secreted by liver & other tissues. The effect of growth hormone on growth, cartilage and protein metabolism depend on interaction between GH & somatomedian.
Short stature, secondary to growth hormone deficiency is associated with –
| A |
Normal body proportion. |
|
| B |
Low birth weight |
|
| C |
Normal epiphyseal development |
|
| D |
Height age equal to skeletal age |
Short stature, secondary to growth hormone deficiency is associated with –
| A |
Normal body proportion. |
|
| B |
Low birth weight |
|
| C |
Normal epiphyseal development |
|
| D |
Height age equal to skeletal age |
Ans. is ‘a’ i.e., Normal body proportion
Short stature due to Human Growth hormone deficiency in characterized by ‑
1. Ratio of upper to lower segment is normal.
2. Bone age or epiphyseal development in less than chronological age by about 2 years.
3. Children’s are normal in height and weight at birth.
4. Delay in growth is usually observed after the age of one year.
Bone age in less than the chronological age in –
o Constitution delay in puberty.
o Marked delayed in hypothyroidism and hypopituitarism.
o Moderate delay in malnutrition and chronic illnesses.
Bone age is advance than height age in
o Down’s syndromes Intrauterine infections
o Turners syndrome
Characteristic features of growth hormone deficiency include all of the following except‑
| A |
Short stature since birth |
|
| B |
Symptomatic hypoglycemia |
|
| C |
Delayed tooth eruption |
|
| D |
Sexual infantilism |
Characteristic features of growth hormone deficiency include all of the following except‑
| A |
Short stature since birth |
|
| B |
Symptomatic hypoglycemia |
|
| C |
Delayed tooth eruption |
|
| D |
Sexual infantilism |
Ans. is ‘a’ i.e., Short stature since birth
The child with hypopituitarism is usually of normal size and weight at birth.
Here is a differential diagnosis of Short stature
See the following table:
|
Constitutional |
Familial short |
Hypopituitarism |
Hypothyroidism |
Turner |
|
Delay |
stature |
|
|
syndrome |
|
+ve |
+ve |
usually –ve |
–ye |
usually –ve |
|
Normal |
Low |
Normal |
Normal |
Low |
|
Slow from |
Slow from |
Slow from a |
Slpw from |
Slow from |
|
infancy |
birth |
few months after birth |
birth |
birth |
|
Moderate |
Normal |
Progressive |
Severe |
Variable |
|
progressive retardation |
|
retardation |
retardation |
|
|
Delayed |
Normal |
Delayed |
Delayed |
Delayed |
|
Normal |
Normal |
Low |
Normal |
Variable |
|
Normal |
Normal |
Low except in isolated GHD |
Variable |
High |
o Family history o Birth weight and height
o Pattern of growth
o Epiphyseal development
o Puberty
o GH levels
o Gonadotropins
Deficiency of growth hormone leads to-
| A |
Delayed fusion of epiphysis |
|
| B |
Proportionate dwarfism |
|
| C |
Acromegaly |
|
| D |
a and b |
Deficiency of growth hormone leads to-
| A |
Delayed fusion of epiphysis |
|
| B |
Proportionate dwarfism |
|
| C |
Acromegaly |
|
| D |
a and b |
Ans. is ‘a’ i.e., Delayed fusion of epiphysis; ‘b’ i.e., Proportionate dwarfism
o Delayed closure of the epiphysis permits growth beyond the normal age when growth should be complete.
o There is proportionate shortening.
Growth hormone secretion is stimulated by ‑
| A |
Increased blood glucose |
|
| B |
Decreased blood glucose |
|
| C |
Cortisol |
|
| D |
Somatostatin |
Growth hormone secretion is stimulated by ‑
| A |
Increased blood glucose |
|
| B |
Decreased blood glucose |
|
| C |
Cortisol |
|
| D |
Somatostatin |
Ans. is ‘b’ i.e., Decreased blood glucose
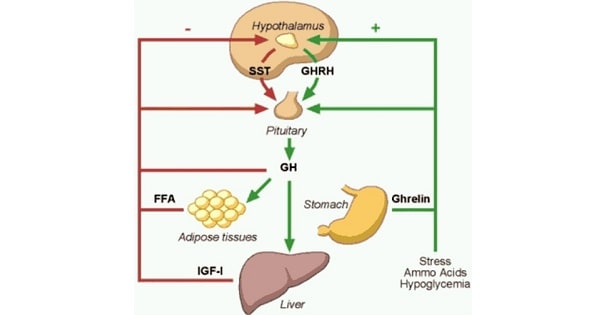
Regulation of GH secretion
GH secretion is regulated by GHRH released from hypothalamus. GH is secreted in a pulsatile fashion throughout the life, with elevated rates of secretion immediately after birth and at puberty. Interestingly, large bursts of secretion occur at night during the onset of deep sleep.
Stimuli that increase secretion of GH are hypoglycemia, exercise, fasting, protein meals, aminoacids (like arginine), stress, glucagon, pyrogen, lysin vasopressin, apomorphins, L-dopa & a-adrenergics, estrogen, androgens and 2-deoxyglucose.
Stimuli that decrease secretion of GH are REM sleep, glucose, Somatostatin, cortisol, FFA, GH itself, IGF-1, and medroxyprogesteron.
Growth hormone secretion is decreased by ‑
| A |
Hypoglycemia |
|
| B |
Exercise |
|
| C |
REM sleep |
|
| D |
Stress |
Growth hormone secretion is decreased by ‑
| A |
Hypoglycemia |
|
| B |
Exercise |
|
| C |
REM sleep |
|
| D |
Stress |
Ans. is ‘c’ i.e., REM sleep
REM sleep decreases the secretion of GH. Other three stimuli increase GH secretion.
Growth hormone has its effect on growth through‑
| A |
Directly |
|
| B |
IG1-1 |
|
| C |
Thyroxine |
|
| D |
Intranuclear receptors |
Growth hormone has its effect on growth through‑
| A |
Directly |
|
| B |
IG1-1 |
|
| C |
Thyroxine |
|
| D |
Intranuclear receptors |
Ans. is ‘b’ i.e., IGI-1
GH has two major functions :-
i) Growth of skeletal system :- The growth is mediated by somatomedins (IGF). Increased deposition of cartilage (including chondroitin sulfate) and bone with increased proliferation of chondrocytes and osteocytes.
ii) Metabolic effects :- Most of the metabolic effects are due to direct action of GH. These include gluconeogenesis, decreased peripheral utilization of glucose (decreased uptake), lipolysis and anabolic effect on proteins.
Growth hormone does not cause ‑
| A |
Gigantism |
|
| B |
Acromegaly |
|
| C |
Diabetes mellitus |
|
| D |
Hypothyroidism |
Growth hormone does not cause ‑
| A |
Gigantism |
|
| B |
Acromegaly |
|
| C |
Diabetes mellitus |
|
| D |
Hypothyroidism |
Ans. is ‘d’ i.e., Hypothyroidism
Physiological effects of Growth hormone
- Growth hormone has two major action, i.e., (1) Stimulation of skeletal growth, and (2) Regulation of metabolism. 3) Stimulation of skeletal growth
The effect of GH on skeletal growth is mediated by somatomedins (Insulin-like growth factors : IGF). They are synthesized mainly in the liver. The growth promoting action of somatomedins is helped by their insulin like actions. GH, through somatomedin (IGF-1), stimulates proliferation of chondrocytes and osteocytes resulting in increased deposition of chondroitin sulfate in catilage and increased ossification of the newly formed cartilage.
GH deficiency in early life causes dwarfism (small height). GH excess in early life leads to gigantism, whereas growth hormone excess in adulthood results in acromegaly.
2) Regulation of metabolism
Protein metabolism : – GH has predominantly anabolic effects on skeletal and cardiac muscle where it promotes amino acid transport into cells and increase protein synthesis.
Carbohydrate and fat metabolism : – The effects of GH on carbohydrate and fat metabolism are complicated by the fact that GH has anti-insulin effects, whereas somatomedins it produces have insulin like effects:-
i) Anti-insulin effects due to direct effect of GH include decreased peripheral utilization of glucose, increased gluconeogenesis, hyperglycemia, and lipolysis. Due to its anti-insulin effects GH excess can cause insulin resistant diabetes mellitus.
ii) Insulin like effects due to somatomedins (IGF) include antilipolytic activity, and other insulin like effects.
