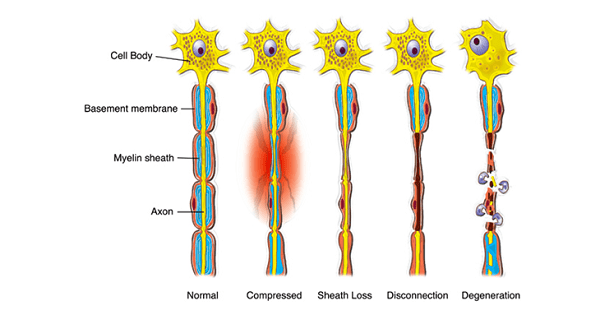
NERVE INJURIES
NERVE INJURIES
- Effects of nerve injury depend upon degree of damage.
Types of neuronal injury:
1. Based on Seddon’s classification,
| Nerve injury type | Injury | Axonal damage | Degeneration | Recovery | Prognosis | Features | Examples |
| NEUROPRAXIA | Temporary injury.
Contusion of peripheral nerve occurs. |
No.
Axon preserved. |
No | Complete recovery | Best | Physiological
conduction block without anatomic disruption. |
Seen in Crutch palsy, Tourniquet palsy, Saturday night palsy. |
| AXONOTMESIS
|
Disrupted axons & myelin.
Intact endoneurium |
Yes.
|
Yes.
|
Spontaneous | Good | Seen in, Closed fracture & Dislocations. | |
| NEUROTMESIS
|
Complete anatomical section of nerve | Yes | Yes | No possible recovery | Bad | Seen in open wound. |
2. Based on Sunderland’s grading of nerve injury:
| I | M/C type, due to ischemia, only transient loss of function, no anatomical disruption |
| II | Prolonged/severe pressure, death of axon locally/ distally |
| III | Interruption of endoneurial tubes |
| IV | Fascicles becoming disorganized |
| V | Complete transection of nerve fibers |
PATHOLOGICAL CHANGES AFTER NERVE INJURY:
- These changes were seen only in Axonotmesis & neurotmesis.
- Not seen in neuropraxia – Due to no anatomical disruption.
NERVE DEGENERATION:
Sequential changes occurring,
Wallerian/Secondary degeneration:
- Secondary degeneration occurring distal to site nerve injury site (within 24hrs).
- Axon degeneration followed by myelin degeneration.
- Axon with its endoneurium initially breaks into small rodlets.
- All debris is cleared by Schwann cells & macrophages, resulting in Ghost tubes formation.
- Intact neurilemma.
Retrograde/primary degeneration:
- Degenerative changes in proximal fragment up to first node of Ranvier.
- Chromatolysis (Breakdown of Nissl granules) – Most Important histological sign of neuronal injury.
- Disappearance of golgi apparatus & neurofibrils.
NERVE REGENERATION:
Distal to injury:
- Rate of axon recovery – 1 mm/day.
Shows “Positive Tinel’s sign” –
- Patient experiencing tingling sensation when skin over nerve is percussed gently from distal to proximal on nerve recovering – Sign for recovery.
- Absent in neuropraxia.
“Motor march” –
- Nearest muscle to injury recovers first followed by other innervated muscles from proximal to distal.
- Seen only in axonotmesis.
Proximal to injury:
- Reappearance of Nissl granules (within 48hrs), neurofibrils & Golgi apparatus.
Note: No regeneration occurs in CNS, because it has no centrosomes.
Exam Important
NERVE INJURIES
Classification:
Based on Seddon’s classification,
| Nerve injury type | Injury | Axonal damage | Degeneration | Recovery | Prognosis |
| NEUROPRAXIA
|
Temporary injury.
Physiological conduction block without anatomic disruption. |
No.
Axon preserved. |
No | Complete recovery | Best |
| AXONOTMESIS
|
Disrupted axons & myelin.
Intact endoneurium |
Yes.
|
Yes.
|
Spontaneous | Good |
| NEUROTMESIS
|
Complete anatomical section of nerve | Yes | Yes | No possible recovery | Bad |
PATHOLOGICAL CHANGES AFTER NERVE INJURY:
- Not seen in neuropraxia – Due to no anatomical disruption.
NERVE DEGENERATION:
1. Wallerian/Secondary degeneration:
- Secondary degeneration occurring distal to site nerve injury site (within 24hrs)
- Axon degeneration followed by myelin degeneration.
2. Retrograde/primary degeneration:
- Chromatolysis (Breakdown of Nissl granules)
- Disappearance of golgi apparatus & neurofibrils.
NERVE REGENERATION:
1. Distal to injury:
- Rate of axon recovery – 1 mm/day.
- Shows “Positive Tinel’s sign” – Absent in neuropraxia.
- “Motor march” – Seen only in axonotmesis.
