NERVE INJURIES
TRUE about neuropraxia is:
| A |
Nerve degeneration present distally + proximally |
|
| B |
Anatomic disruption of the nerve fibre occurs |
|
| C |
Reversible physiological nerve conduction block |
|
| D |
Recovery does not occur |
TRUE about neuropraxia is:
| A |
Nerve degeneration present distally + proximally |
|
| B |
Anatomic disruption of the nerve fibre occurs |
|
| C |
Reversible physiological nerve conduction block |
|
| D |
Recovery does not occur |
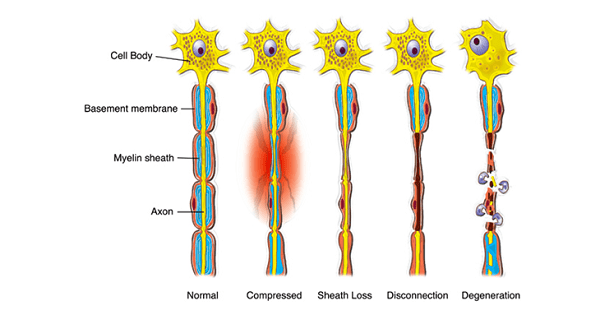
Nerve injuries are of three types:
1. Neuropraxia: In neuropraxia there is reversible physiological nerve conduction block with no anatomical disruption of nerve fibre. There is no degeneration of nerve fibre and recovery completes within 6 weeks.
2. Axonotmesis: In this type of nerve injury there is loss of conduction due to axonal interruption but the nerve is in continuity and the neural tubes are intact. Degeneration is present distally as well as proximally and neuromas present in continuity. Recovery is +/-.
3. Neurotmesis: In this type of nerve injury there is complete division of nerve ( i.e epineurium and axons all have lost their continuity). Degeneration is present distally as well as proximally and end neuromas are present. Recovery is poor without surgical intervention.
Ref: Apley’s 8/e, page 233.
Difference between neuropraxia and neuronotomesis is:
| A |
EMG finding |
|
| B |
Sensory loss |
|
| C |
Motor loss |
|
| D |
All |
Difference between neuropraxia and neuronotomesis is:
| A |
EMG finding |
|
| B |
Sensory loss |
|
| C |
Motor loss |
|
| D |
All |
A i.e. EMG finding
Axonotmesis includes discontinuity in:
| A |
Perineurium |
|
| B |
Epineuri um |
|
| C |
Endoneurium |
|
| D |
Axon |
Axonotmesis includes discontinuity in:
| A |
Perineurium |
|
| B |
Epineuri um |
|
| C |
Endoneurium |
|
| D |
Axon |
D i.e. Axon

Neuronal degeneration is seen in all of the following except:
| A |
Crush nerve injury |
|
| B |
Fetal development. |
|
| C |
Senescence |
|
| D |
Neuropraxia |
Neuronal degeneration is seen in all of the following except:
| A |
Crush nerve injury |
|
| B |
Fetal development. |
|
| C |
Senescence |
|
| D |
Neuropraxia |
D i.e. Neuropraxia
Neuropraxia refers to physiological disruption of conduction only, no structural changes or degeneration occur. Neuronal degeneration is seen inQ – Crush nerve injury, Fetal development, Senescence
Seddon’s Classification of Nerve Injury
|
Features |
Neuropraxia |
Axontemesis |
Neurontemesis |
|
Pathology |
– No anatomical disruption |
Axons & myelin sheath disrupted but |
– Complete division of nerve |
|
|
– Both axon & sheath intact – Physiological disruption of |
endoneural perineurium and epineurium sheath (neural tube) is |
– Axon & neural tube (i.e. perineurium, epineurium, & endoneural sheath) |
|
|
conduction only |
intactQ |
both are divided. |
|
Degeneration |
No degeneration Q |
Degeneration present proximal + distal |
Degeneration present proximal + Distal |
|
|
|
(Wallerian) |
(Wallerian) |
|
Neuroma |
No |
In continuity |
End or side neuroma |
|
Tinel’s sign12/ |
Absent |
Advancing (present) |
Static |
|
Motor march |
|
|
|
|
Prognosis |
– Excellent |
– Good /fair /poor |
Poor |
|
|
– Recovery is complete usually with in 6 weeks |
– Occurs as regenerating axons grow into intact sheath |
|
– Electrodiagnostic studies (like nerve conduction study & EMG) are used to distinguish between partial & complete lesionQ and to establish a baseline for monitoring subsequent functional recoveryQ. However, these are not helpful until 2-3 weeks after an acute injury.
– If a muscle lose its nerve supply (d/t nerve injury), EMG shows denervation potential at 3rd week; which exludes neuropraxia but however does not differentiate between axontmesis and neu rontemesis.
All types of injuries may cause sensory, motor or both loss depending on type of nerve damaged.
* Each axon is covered by myelin sheath (in myelinated nerve only) &/or neurilemma (Schwann sheath). Each nerve fiber (containing many axons) is covered by endoneurium. Each fasciculus (containing many nerve fibres) is covered by perineurium. And each nerve (containing mamy fasciculus) is covered by epineurium.
Neuropraxia is defined as:
March 2012
| A |
Anatomically normal but physiological interruption of nerve conduction |
|
| B |
Nerve intact with broken axons |
|
| C |
Axons as well as nerve broken |
|
| D |
None of the above |
Neuropraxia is defined as:
March 2012
| A |
Anatomically normal but physiological interruption of nerve conduction |
|
| B |
Nerve intact with broken axons |
|
| C |
Axons as well as nerve broken |
|
| D |
None of the above |
Ans: A i.e. Anatomically normal but physiological interruption of nerve conduction
Sunderland classification is used for ‑
| A |
Nerve injury |
|
| B |
Muscle injury |
|
| C |
Tendon injury |
|
| D |
Ligament injury |
Sunderland classification is used for ‑
| A |
Nerve injury |
|
| B |
Muscle injury |
|
| C |
Tendon injury |
|
| D |
Ligament injury |
Ans. is ‘a’ i.e., Nerve injury
Sunderland is an extension of the seddon classification and includes 5 types of nerve injuries.
Tinel sign is seen in ‑
| A |
Nerve degeneration |
|
| B |
Nerve regeneration |
|
| C |
Muscle degeneration |
|
| D |
Muscle regeneration |
Tinel sign is seen in ‑
| A |
Nerve degeneration |
|
| B |
Nerve regeneration |
|
| C |
Muscle degeneration |
|
| D |
Muscle regeneration |
Ans. is ‘b’ i.e., Nerve regeneration
Pathological changes after nerve injury
- After nerve injury, nerve first degenerates and then tries to regenerate.
Nerve degeneration
- The part of the neurone distal to the point of injury undergoes secondary or Wallerian degeneration; the proximal part undergoes primary or retrograde degeneration upto a single node.
Nerve regeneration
- As regeneration begins, the axonal stump from the proximal segment begins to grow distally. If the endoneural tube with its contained Schwann cells is intact, the axonal sprout may readily pass along its primary course and reinnervate the end-organ. The rate of recovery of axon is 1 mm per day. The muscles nearest to the site of injury recovers first, followed by others as the nerve reinnervates muscles from proximal to distal, the so-called motor march.
- When the skin over the nerve is percussed gently from distal to proximal, the patient gets a tingling sensation if the nerve is recovering. This is called Tinel’s sign and is a sign of recovery.
Physiological interruption of transmission is ‑
| A |
Neuropraxia |
|
| B |
Neurotmesis |
|
| C |
Axonotmesis |
|
| D |
None of the above |
Physiological interruption of transmission is ‑
| A |
Neuropraxia |
|
| B |
Neurotmesis |
|
| C |
Axonotmesis |
|
| D |
None of the above |
Ans. is ‘a’ i.e., Neuropraxia
Seddon’s classification of nerve injuries
- Seddon identified three types of injuries
1) Neuropraxia
- There is contusion of the peripheral nerve which causes reversible physiological nerve conduction block. The axis cylinder (i.e., axon with its endoneurium) is preserved. Thus, there is physiological conduction block without anatomic disruption. The injury is temporary and recovery is complete. It is seen in crutchpalsy, tourniquet palsy, and saturday night palsy.
2) Axonotemesis
- There is injury to axon but endoneurium is preserved. Spontaneous recovery is expected in some cases. This is seen in closed fractures and dislocations.
3) Neurotemesis
- There is complete anatomical section of nerve. No recovery possible. It is seen in open wound.
True regarding nerve injury is:
| A |
In all cases of open wound with clinical signs of nerve injury, nerve exploration should always be done |
|
| B |
Nerve conduction velocity is best predictor within 48 hours of injury |
|
| C |
Positive Tinel’s sign indicates the accurate location of lesion |
|
| D |
Traction nerve injury should be repaired immediately |
True regarding nerve injury is:
| A |
In all cases of open wound with clinical signs of nerve injury, nerve exploration should always be done |
|
| B |
Nerve conduction velocity is best predictor within 48 hours of injury |
|
| C |
Positive Tinel’s sign indicates the accurate location of lesion |
|
| D |
Traction nerve injury should be repaired immediately |
Ans. a. In all cases of open wound with clinical signs of nerve injury, nerve exploration should always be done
Indications of Exploration in Nerve Injuries: (Apley’s 9/e p274)
- Nerve was seen to be divided and needs to be repaired, i.e., open injury
- If the type of injury (example a knife wound or high energy injury) suggest that the nerve has been divided or severely damaged.
- If recovery is inappropriately delayed and diagnosis is in doubt.
- Positive Tinel’s sign tells about the regeneration of the nerve (does not indicates the accurate location of lesion) Traction nerve injury are usually neuropraxia (managed conservatively, should not be repaired immediately)
Nerve Injury
Neuropraxia
- Reversible physiological nerve conduction blockQ
- Seen in crutch palsy, tourniquet palsy, and Saturday night palsyQ
Axonotemesis
- Loss of conduction due to axonal interruptionQbut the nerve is in continuity and the neural tubes are intact
- Seen in closed fractures and dislocations
Neurotemesis
- There is complete division of nerve° (epineurium, perineurium, endoneurium and axon all lost their continuity)
- Seen in open wounds
Nerve Repair
- A clean cut nerve is best repaired as soon as this can be done safelyQ.
- The higher (proximal) the lesion, the worse the prognosisQ.
- Pure motor or pure sensory nerves recover better than mixed, because there is less chances of axonal confusion.
- Tinel’s sign indicate regeneration of nerveQ
- Rate of regeneration of nerve is 1mm/dayQ
Prognosis after Nerve Suturing
- Radial nerve (best)° >Median nerve >Ulnar nerve >Peroneal nerve >Sciatic and femoral nerve (worst prognosis)Q.
