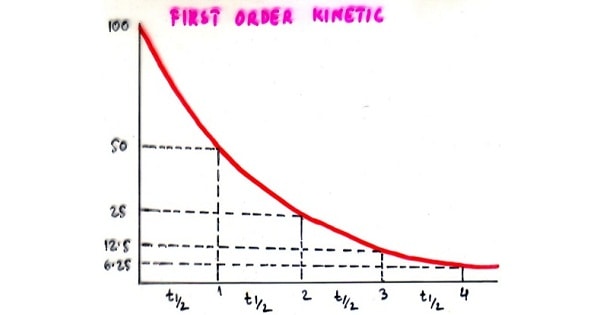
Order Of Kinetics
Order Of Kinetics FIRST ORDER KINETICS: Absorption, distribution, biotransformation and excretion processes are mostly occurring at rates proportional to plasma drug concentration. A constant fraction of drug is absorbed, distributed, biotransformed and excreted per unit time. These processes increase in rate with increase in conc. and decrease with falling conc. A constant fraction of drug in body is eliminated per unit […]